 Notes: NEUROANATOMY NUCLEI SUMMARY
Notes: NEUROANATOMY NUCLEI SUMMARY
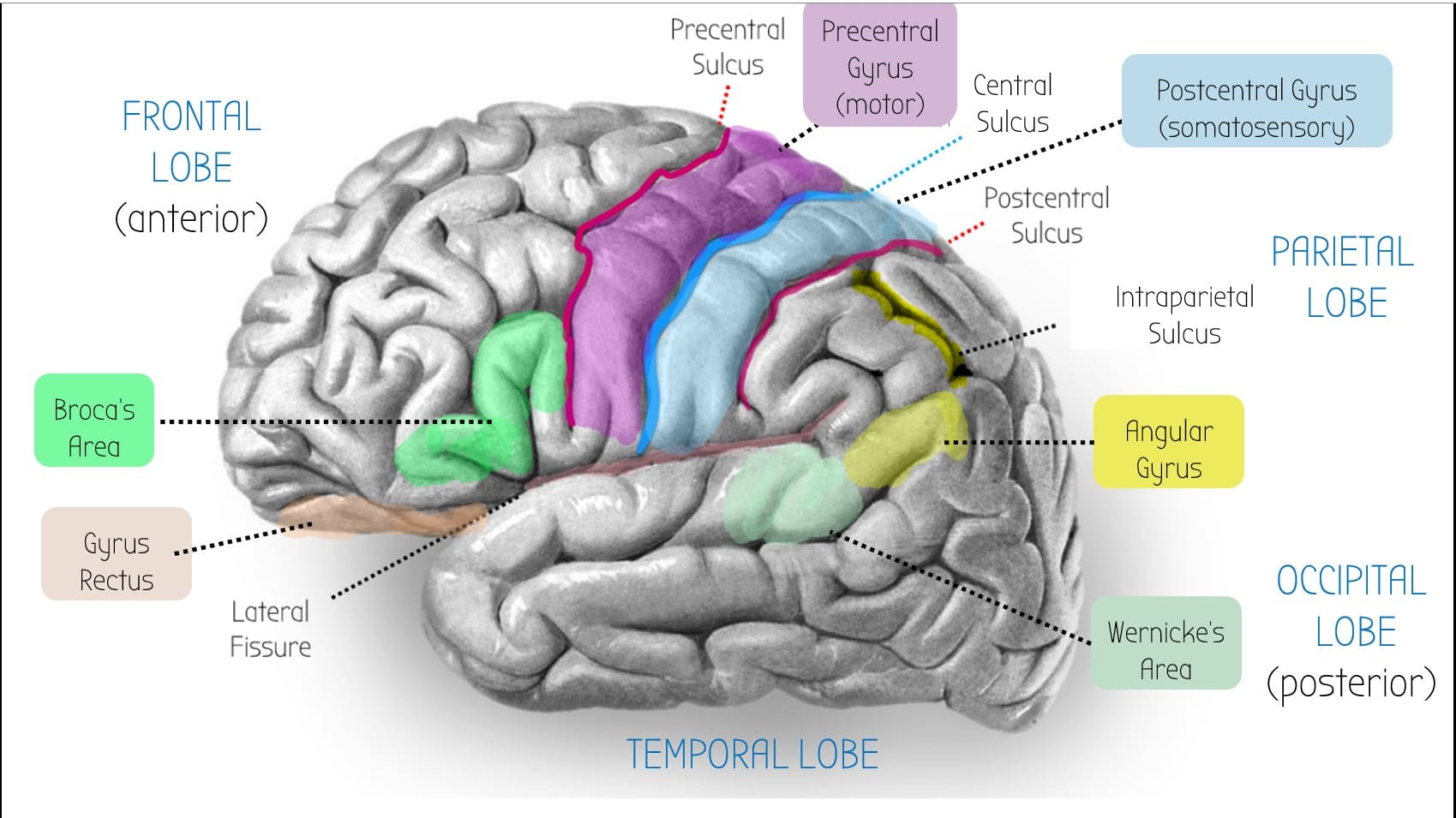
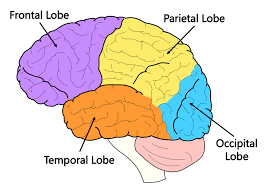
Parietal lobe
--> Dominant side (usually left hemisphere): wernicke's area, broca's area, angular gyrus: language stuff
--> Non-dominant side (usually right hemisphere): spatial processing e.g. constructional ability
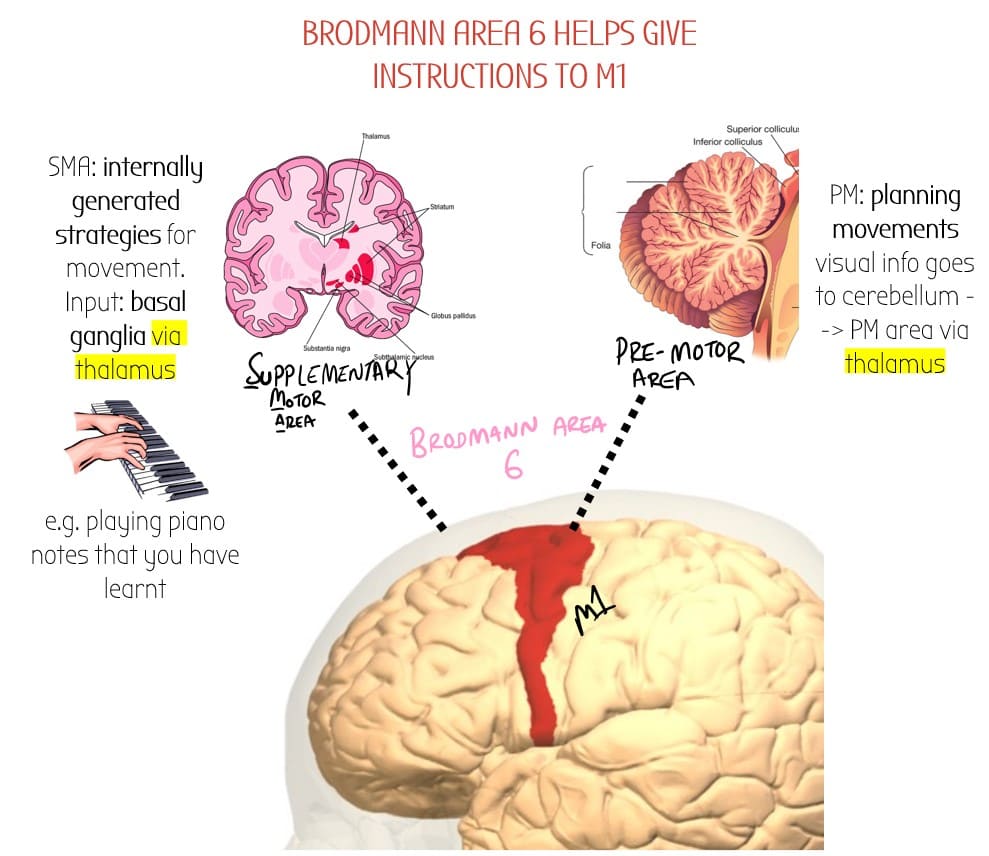
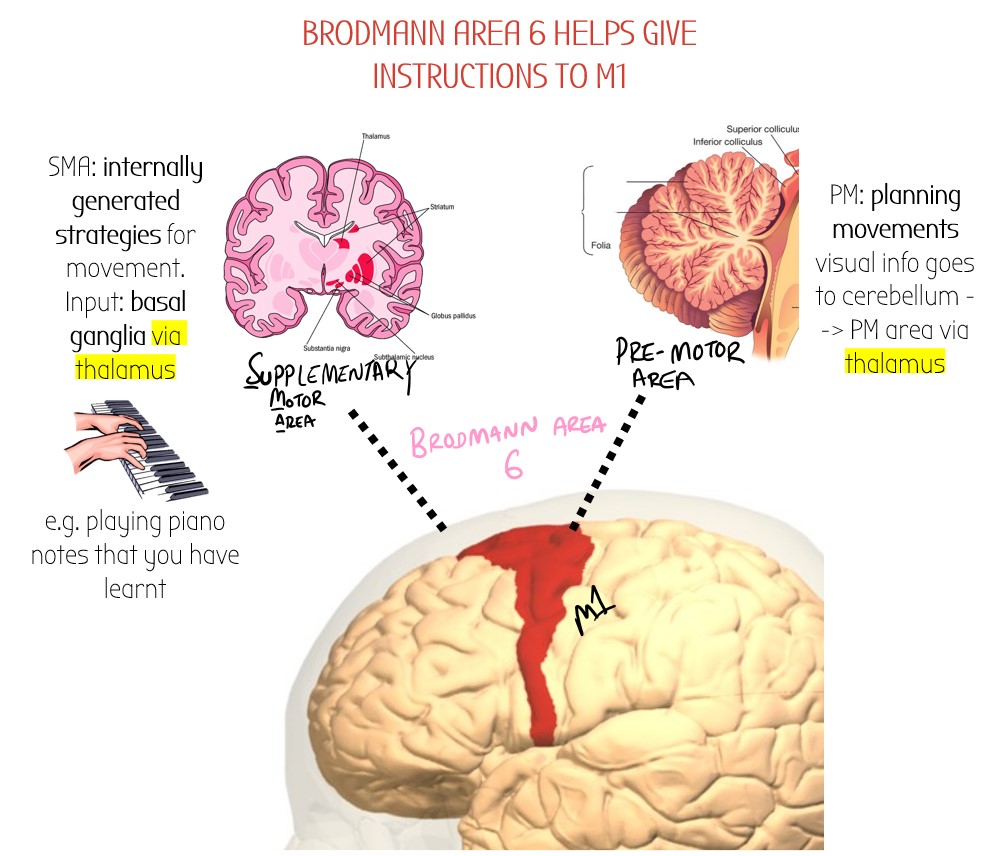
Brodmann area 6
Just anterior to M1 is Brodmann area 6 - an area which assists with motor control.
It is split into:
- Supplementary Motor Area (SMA)
- Premotor Area (PM)
Postcentral Gyrus (S1)
-Main somatosensory area
-inputs: medial leminscus (conscious proprioception) & spinothalamic tract (nociception)
Superior Parietal Lobule
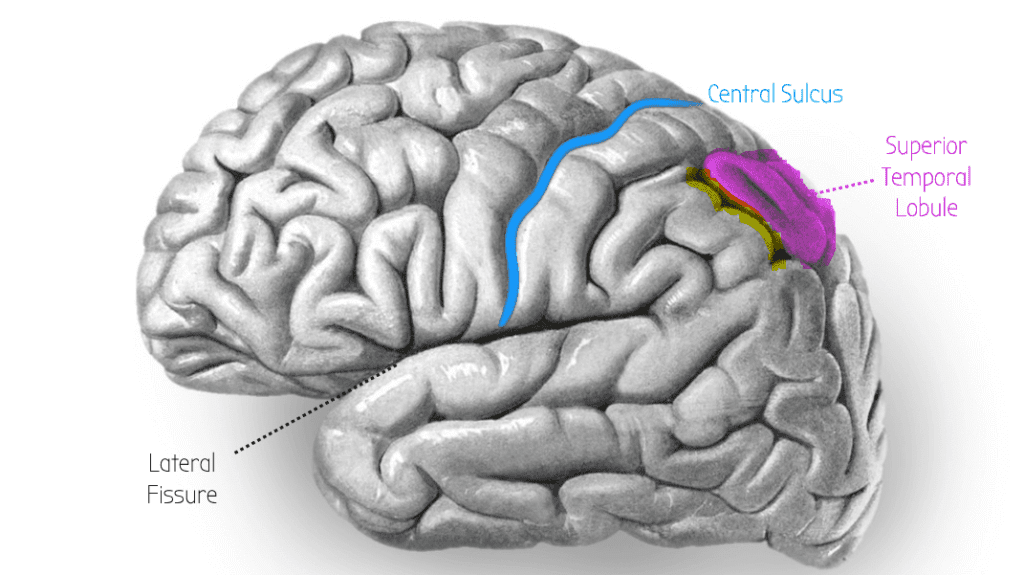
👀 Visual processing - WHERE OBJECTS ARE
--> Info comes from main visual cortex V1 (occipital lobe)
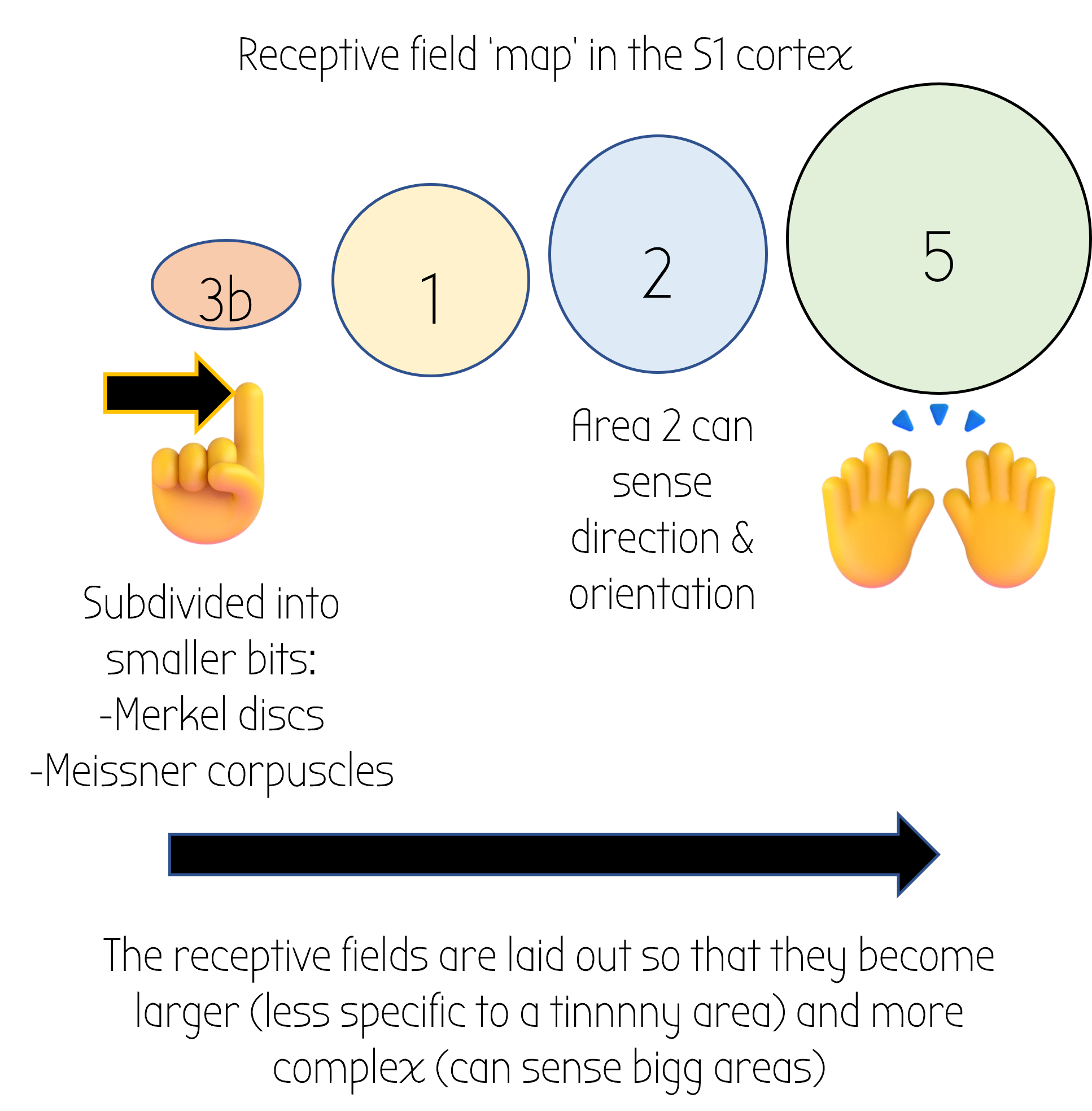
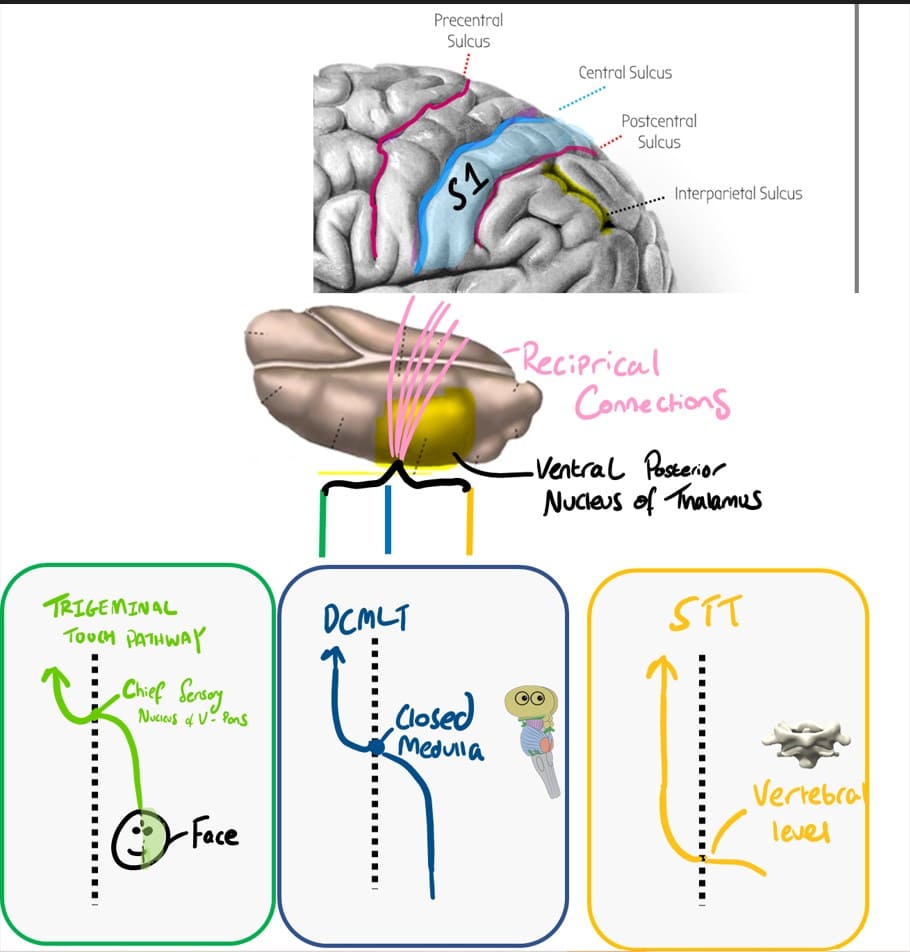
INPUT: TRACTS VIA VP NUCLEUS OF THALAMUS
Several tracts. These first go to the ventral posterior (VP) nucleus of the thalamus and then go to S1 via reciprocal connections.
e.g.
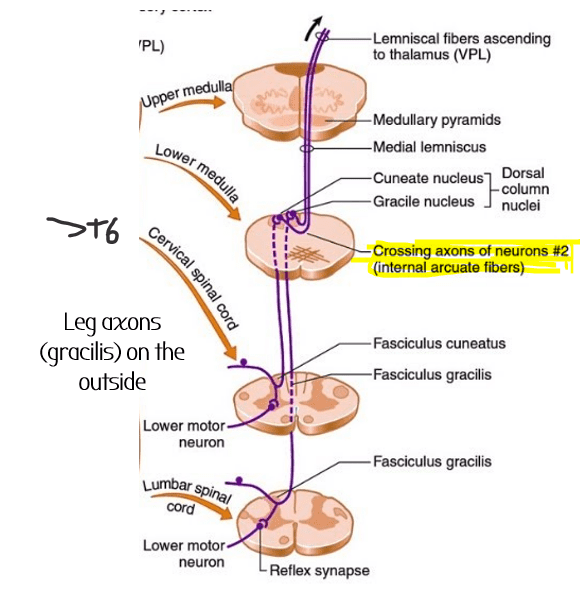
- DCMLT – dorsal column medial lemniscus – conscious proprioception
- Spinothalamic tract – nociception
- Trigeminal touch pathway – column pathway for the face. Fibres project to trigeminal principal sensory nucleus, cross at the midline
INPUT:
Pontocerebellum (lateral bits of cerebellum) –> dentate nucleus in cerebellum via the Ventrolateral thalamus:
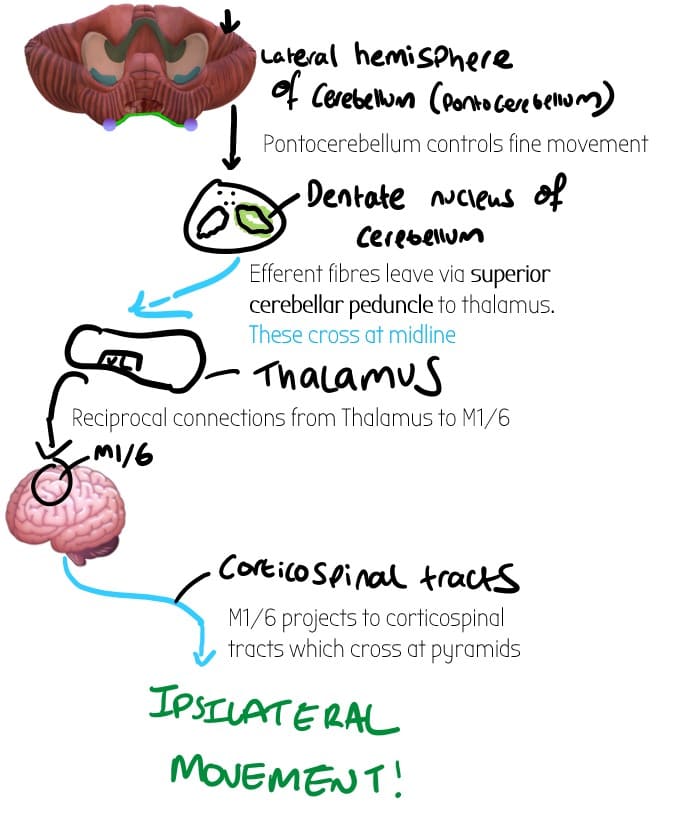
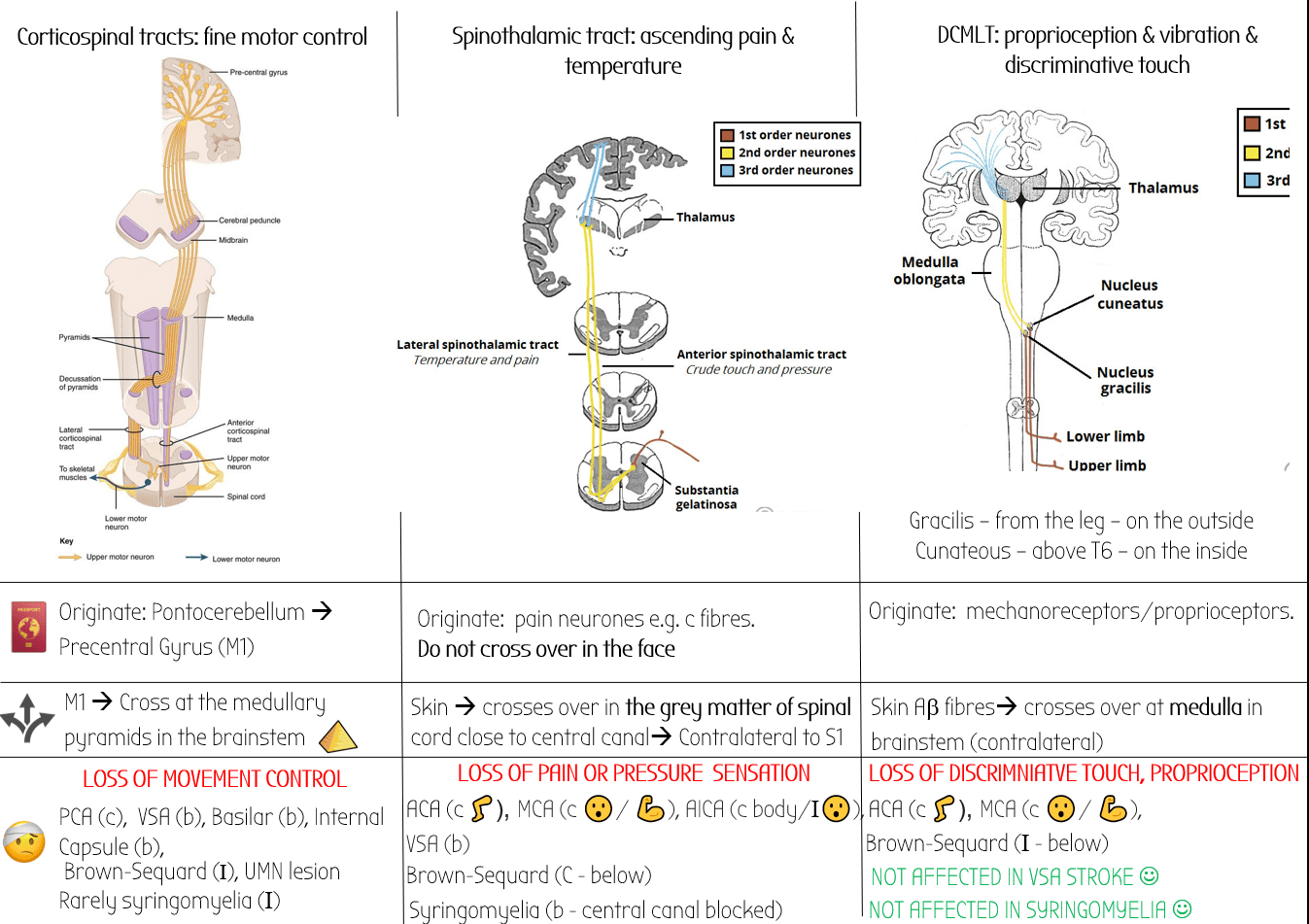
OUTPUT: Corticospinal tracts – cross at pyramids = contralateral
–> Contralateral movement from the M1 (but ipsilateral if you trace all the way to the cerebellum). – Audio explanation below:
Non-Dominant side (usually right hemisphere):
Spatial reasoning
- Right parietal lobe is also responsible for body image. Lesion = you dont recognise your own hand as yours!
- Constructional ability– Make stuff. Lesion = cannot put 3 -piece jigsaw puzzle together
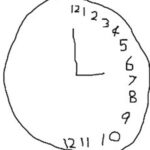
- Lesions in R lobe can also lead to hemineglect – you brain just doesn’t see one side of the world as being there – spoooky!
This makes patients draw stuff like this:
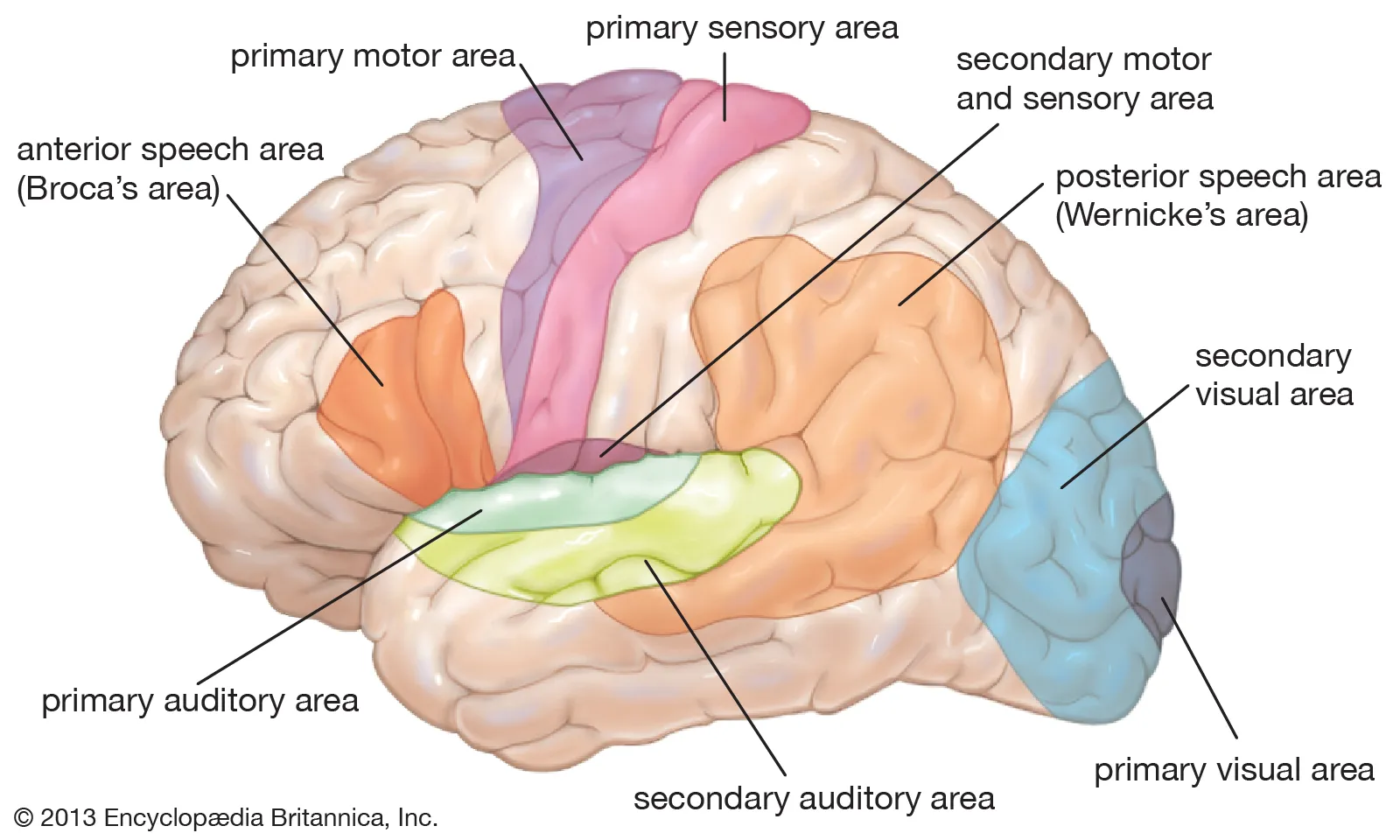
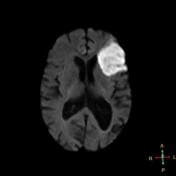
Dominant frontal lobe (shown in orange)
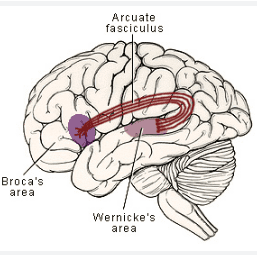
Connected to the wernick’es area by fibres called the arcuate fasiculus
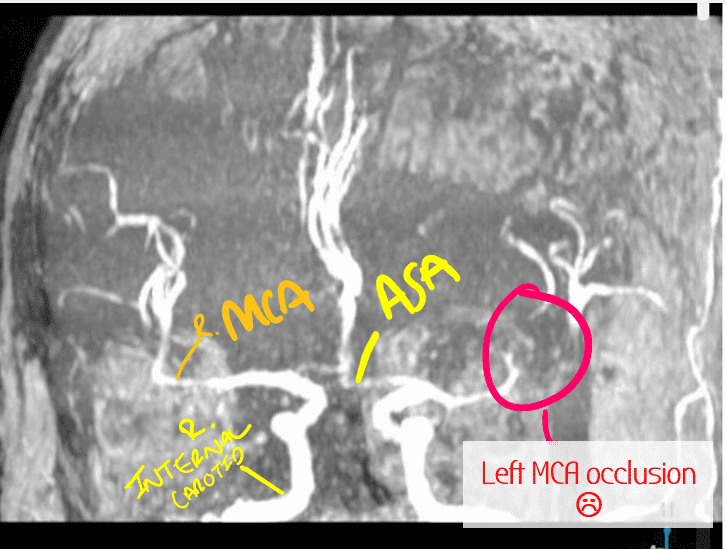
🩸 Supplied by superior division of MCA
MCA Stroke in Broca’s area = expressive aphasia:
-speech is very reduced with limited vocab
-very hard to make out proper sounds- speech is very jumbled
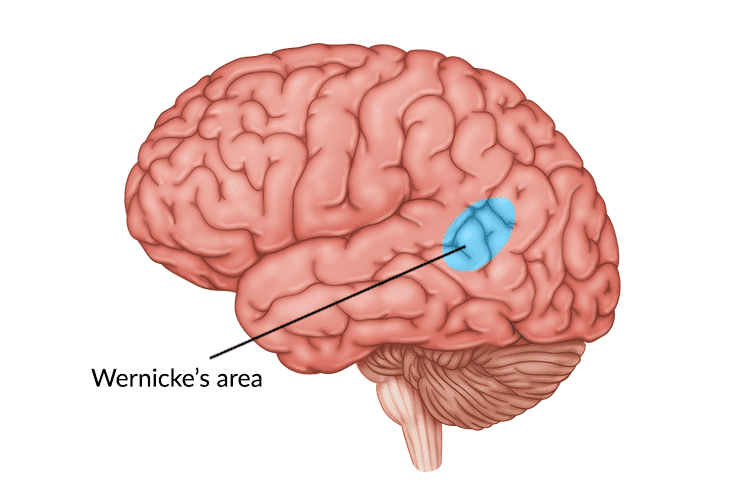
Dominant (usually left) temporal lobe
Connected to the Broca’s area by fibres called the arcuate fasiculus
Also connected to auditory cortex to help understand sounds
 Supplied by inferior division of MCA
Supplied by inferior division of MCA
MCA Stroke in Wernicke’s area = fluent/receptive aphasia:
-Words come out and can be heard but they don’t make any sense
-Words are random like a word salad.
-Also patient may struggle to understand words – poor comprehension 🙁
Parietal lobule
Supplied by inferior division of MCA
Can understand and speak well BUT difficulty in repeating words
=CONDUCTION APHASIA
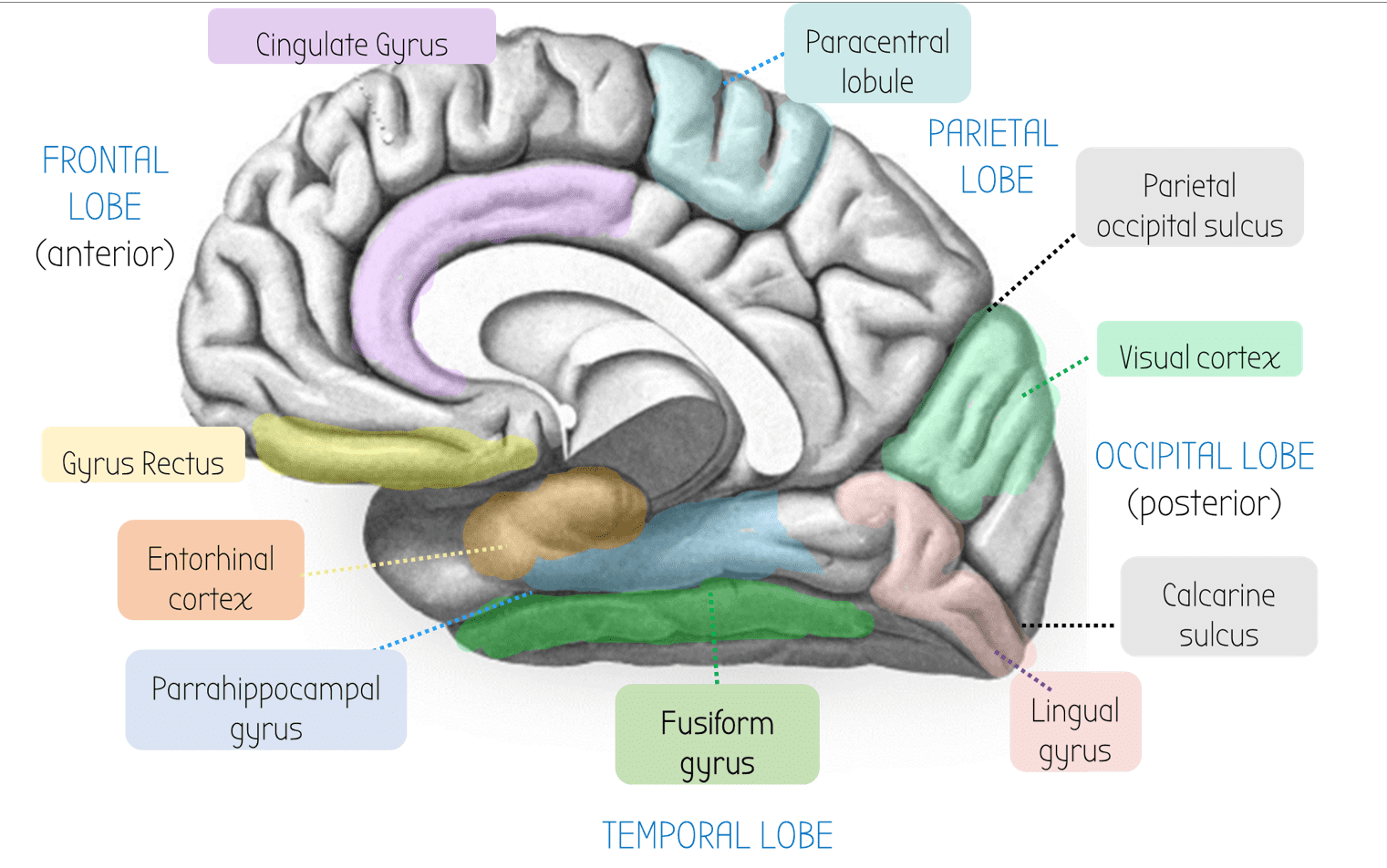
Visual Cortex
At the occipital lobe - supplied by the PCA
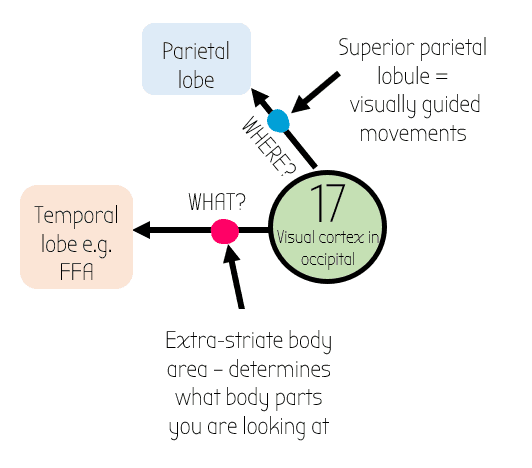
Connected to other parts of the brain
–> Goes up to parietal lobe for the WHERE? info
–> Goes across to temporal lobe for the WHAT lobe e.g. extrastriate body area & Fusiform Face Area
Receives info from reciprocal connections from Lateral Geniculate Nucleus LGN
Supplied by PCA
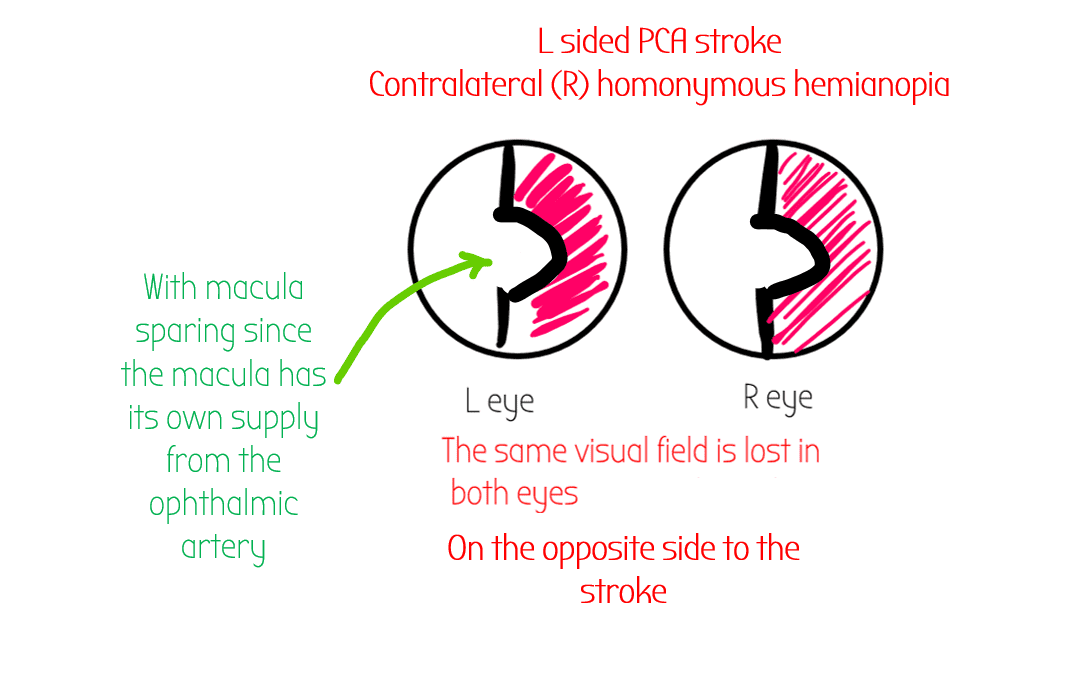
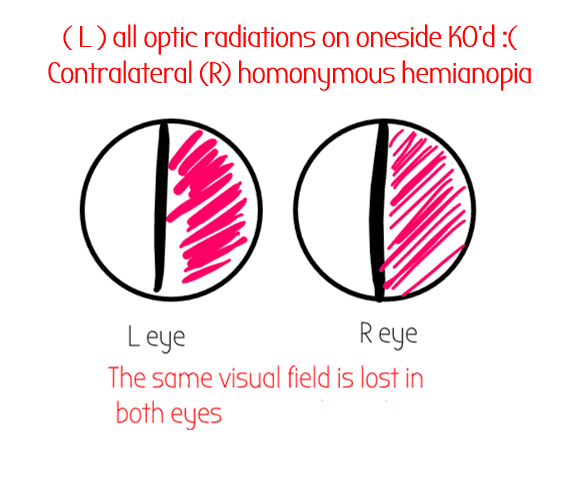
-PCA Stroke (below is a LEFT sided pca stroke – remember brain scans are always flipped)
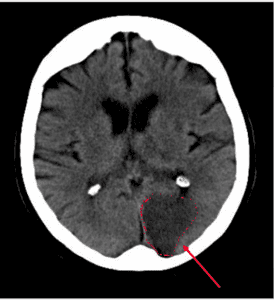
PCA stroke causes contralateral homonymous hemianopia (lost opposite to stroke half the visual field in both eyes ) WITH macular sparing
- Macula has its own supply from the ophthalmic artery (branch of ICA)
PCA stroke may also affect CNIII (oculomotor) – Weber’s Syndrome – Ipsilateral enlarged pupil and ptosis, down and out gaze – so recti don’t work and overpowered by SO & LR
Supplied by PCA
-PCA Stroke / lesion can cause problems in recognising faces – prosopagnosia
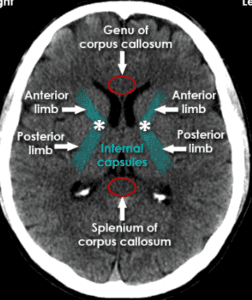
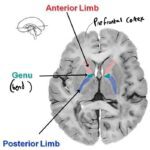
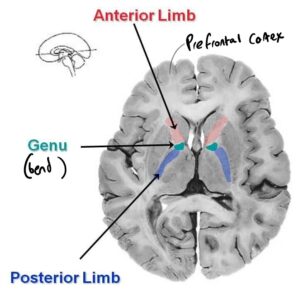
Internal Capsule
-not part of BG
-Posterior limb really important for movement
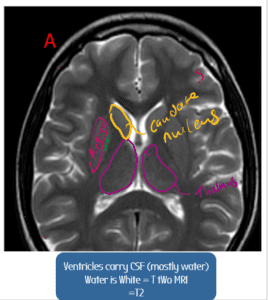
Axial MRI of Basal Ganglia
Listen to the audio explanation here:
Listen to the audio explanation here:
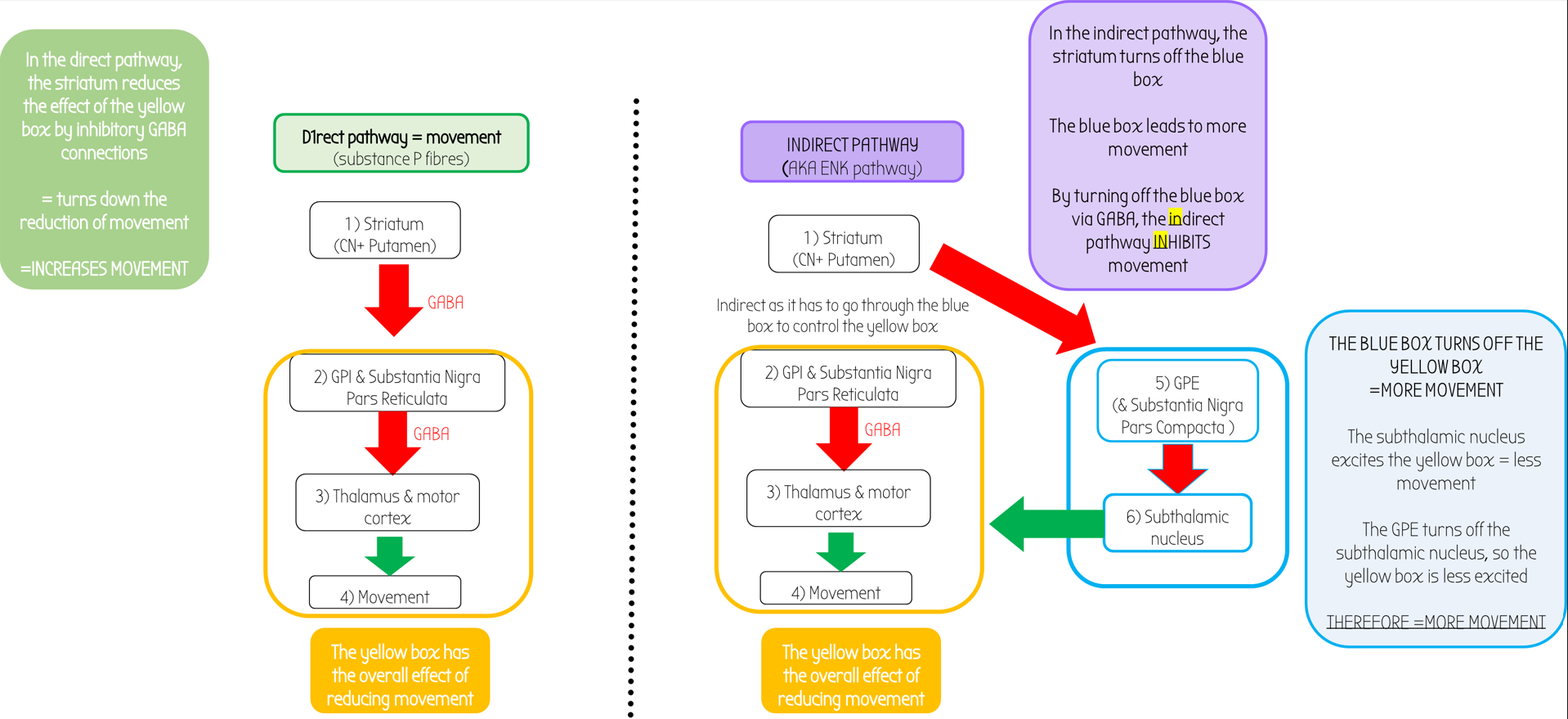
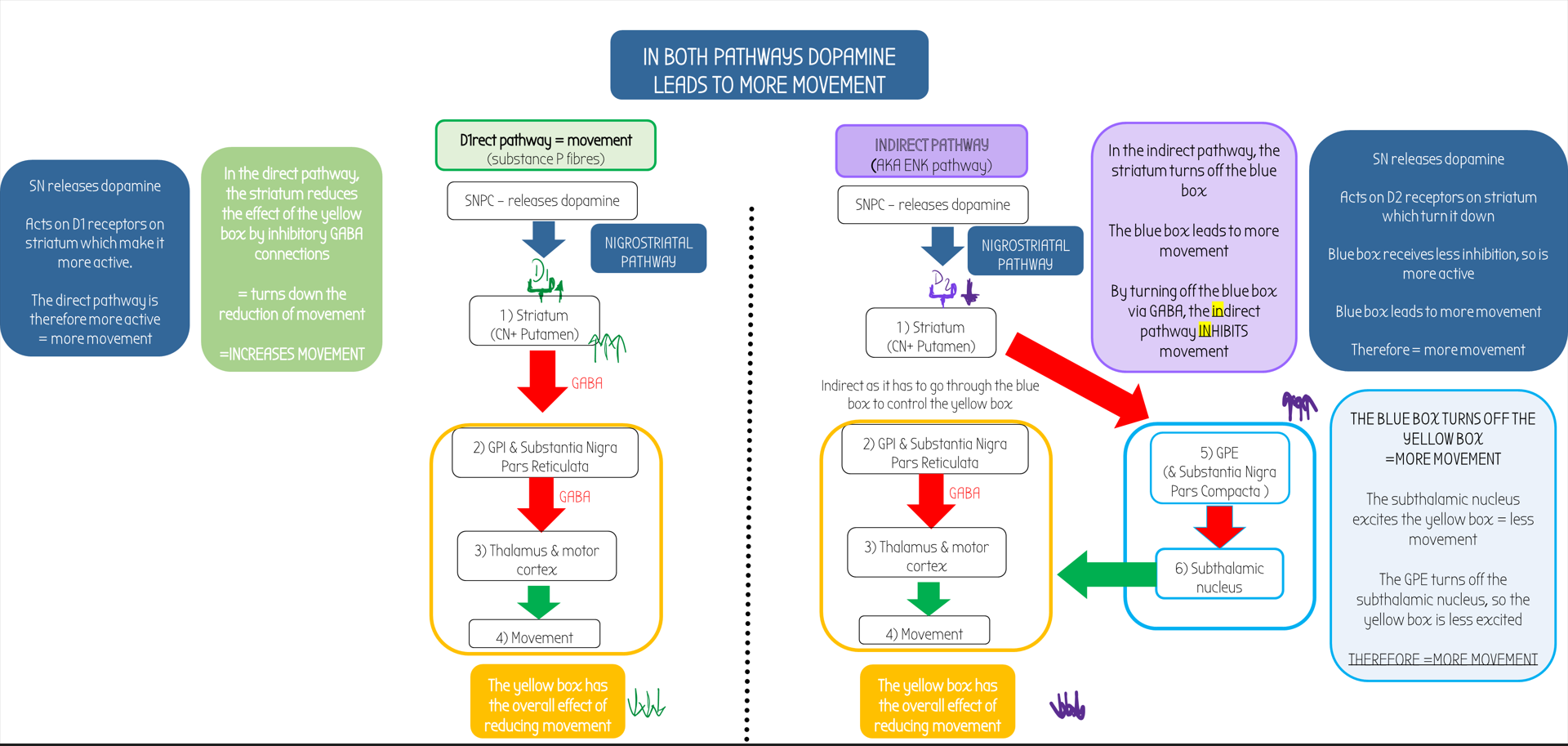
- Dopamine leads to more movement in both pathways
- Often, mutations in the SNCA gene lead to the alpha-synuclein protein to misfold and become sticky
- These naughty proteins can aggregate into evil blobs called Lewy bodies
- Lewy bodies accumulate in SN & damage SN
- =LESS DOPAMINE PRODUCED
therefore lack of dopamine = less movement & problems initiating movement
-Direct pathway less active
-Indirect pathway more active
Parkinsonism may also be due to strokes to areas that supply SN
-e..g paramedian branch of basilar artery (causes Weber’s Syndrome)
contralateral parkinsonism (basal ganglia supply the motor area, then the fibres cross over)
As the problem is lack of dopamine, the main treatment is to give L-DOPA, a precursor to dopamine
- It is able to cross the Blood Brain Barrier (BBB)
 Converted by DOPA decarboxylase from L-DOPA –> Dopamine
Converted by DOPA decarboxylase from L-DOPA –> Dopamine
Side effects of dopamine (L-DOPA) therapy:
The enzyme Dopamine B hydroxylase turns dopamine into NA. This can displace NA from from neurones –> can lead to HYPOTENSION (low bp)
 Also can reduce prolaction (lactating is normally kept under brakes by dopamine. Giving more dopamine can reduce breast milk flow )
Also can reduce prolaction (lactating is normally kept under brakes by dopamine. Giving more dopamine can reduce breast milk flow ) May also cause psychosis
May also cause psychosis L DOPA can act in periperal chemoreceptors and cause nausea
L DOPA can act in periperal chemoreceptors and cause nausea
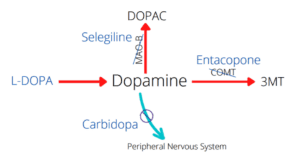
L-DOPA can act on peripheral dopamine receptors and cause nausea. There are two drugs (one works outside the brain – carbidopa, one inside the brain – domperidone) we can use to stop the effects of nausea:
- Carbidopa + benserazide (work outside brain) : inhibit peripheral breakdown of L-DOPA by dopamine DECARBOXYLASE. This means that less L-DOPA is needed to be delivered as less is wasted. As less is in the system, there is a lessened chance of side effects!
- Domperidone (works inside brain) – D2 receptor antagonist. The Chemoreceptor Trigger Zone (CTZ) is in the brainstem and dopamine acts on it to make you feel sick. Domperidone blocks this D2 activation of CTZ and therefore stops you from being sick.
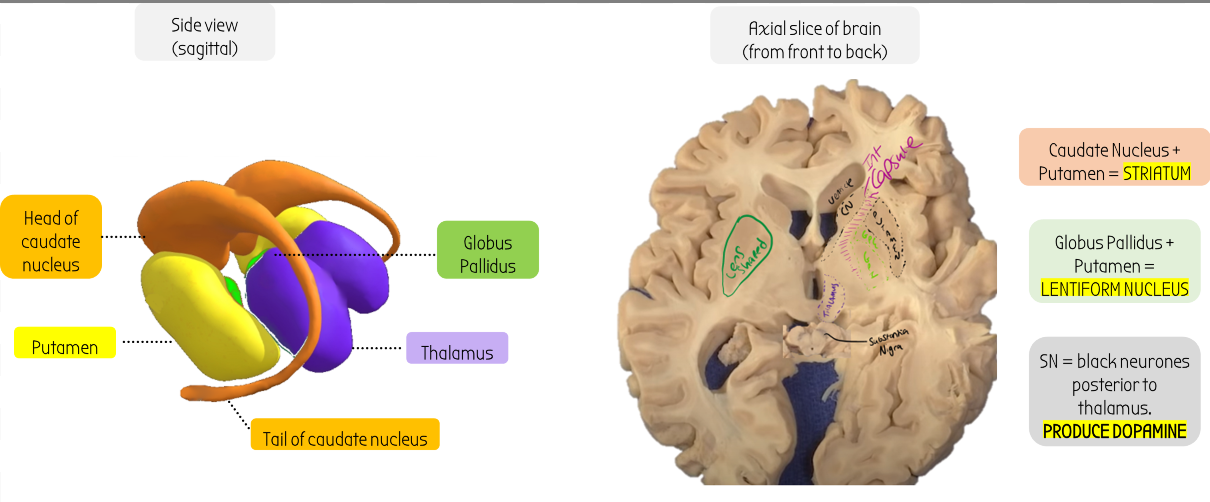
CN & Putamen
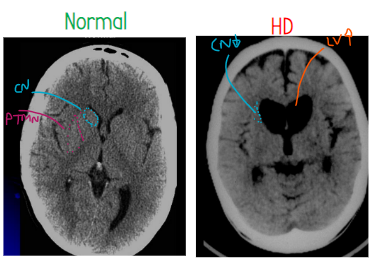
–CN (in blue) & Putamen (pink) atrophied
-Space filled by enlarged lateral ventricles (LV in orange)
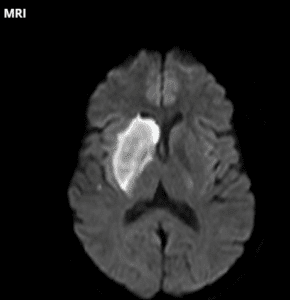
💊 The striatum has a nucleus in it called the nucleus accumbens which responds to cocaine and causes addiction! (don’t take coke all the time)
🩸Striatum is supplied by striate arteries (branch of MCA which comes from internal carortid) which also supplies the internal capsule. Ischaemia (blockage) in striate arteries = LACUNAR STROKE. Usually causes complete contralateral hemiparalysis (e.g. in this example, paralysis of the LEFT side of the body)
😟 Huntigton’s disease: hyperkinetic, jerky movements
-initially degeneration of indirect pathway (
Not part of the basal ganglia but can be seen in the same cross sections.
A passage for fibres to pass through. The anterior bend (‘limb’) of the internal capusle contains the fibres for worrying about stuff.
The posterior limb contains fibres for movement of the contralateral side of the body
Posterior limb:
🩸Supplied by striate arteries that come from middle cerebral artery (which in turn come from internal carotid).
ALL descending contralateral motor neurons are found here.
These striate arteries also supply corpus-striatum, caudate nucleus & striatum
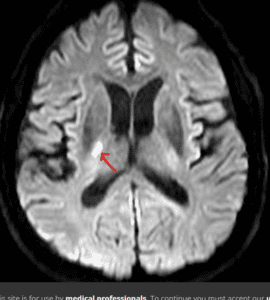
Stroke here (lacunar stroke) can lead to paralysis of the whole body!
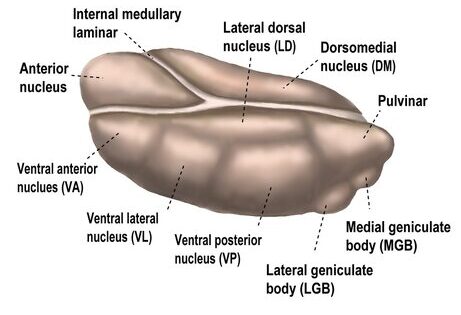
Pulvinar
Has connections with parietal lobe & some of occipital lobe
Dorsal medial nucleus of thalamus
Personality & Emotions
INPUT:
Amygdala
OUTPUT:
Prefrontal cortex - fibres pass through the anterior limb of internal capsule
- Receive info from amygdala (emotion)
- Output fibres go through the anterior limb of the internal capsule, to the prefrontal cortex (front bit of the brain, controls emotions)
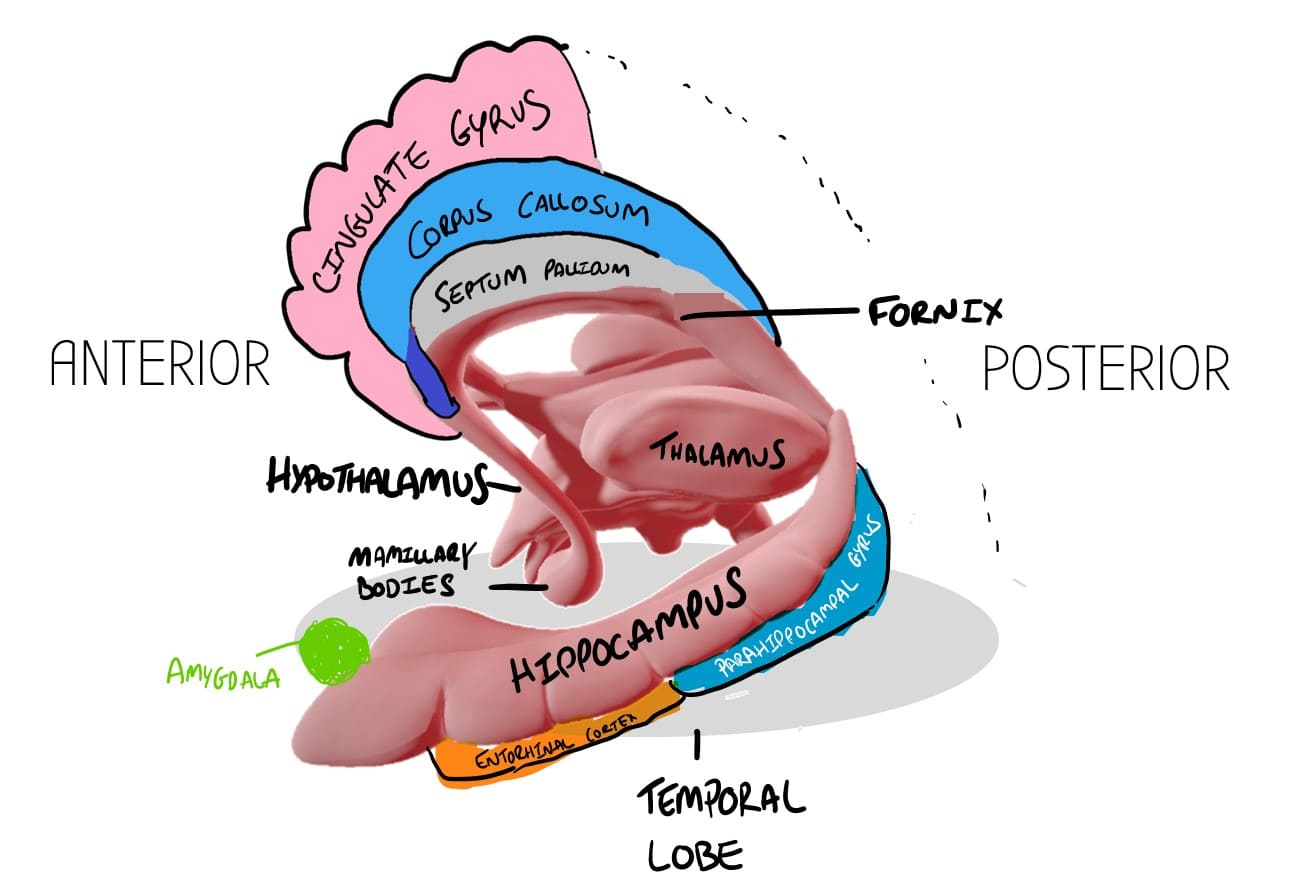
Septum Pellucidum
Makes up the base of the lateral ventricles. There are four ventricles in the brain, two in each hemisphere, a third one that joins them together in the middle, and the 4th ventricle which drains into the cerebral aqueduct which connects to the spinal cord. 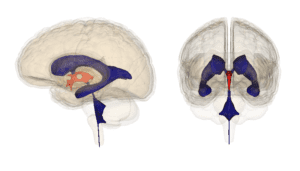
Ventricles drain CSF around the brain
Anterior Commisure
Bit of white matter that connects both hemispheres.
Its close to the nose - olfactory processing/smell occurs here.
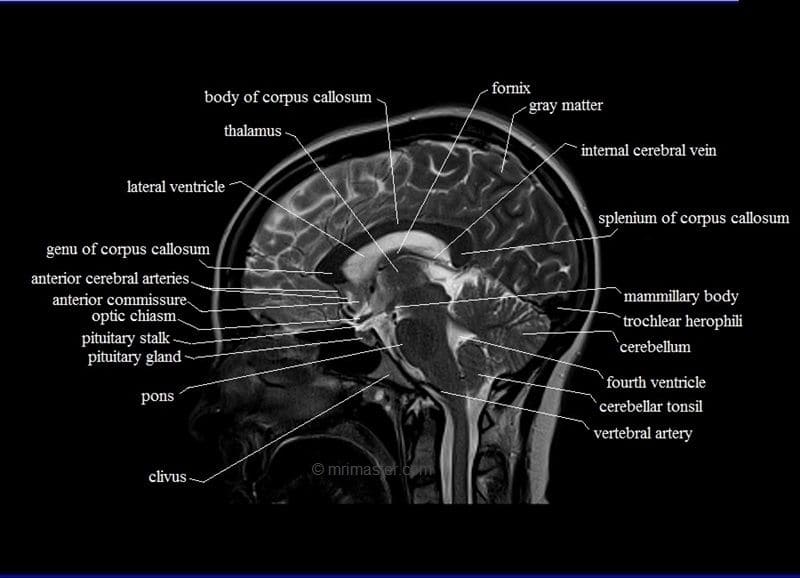
Mamillary Body

At the anterior end of the fornix, where it joins onto the hypothalamus, there are two bulbs which make up the mamillary bodies.
Function: Recollective Memory
🍷 Damaged by alcohol causing problems in memory: Korsakoff's syndrome 🙁
Hippocampus 🦛
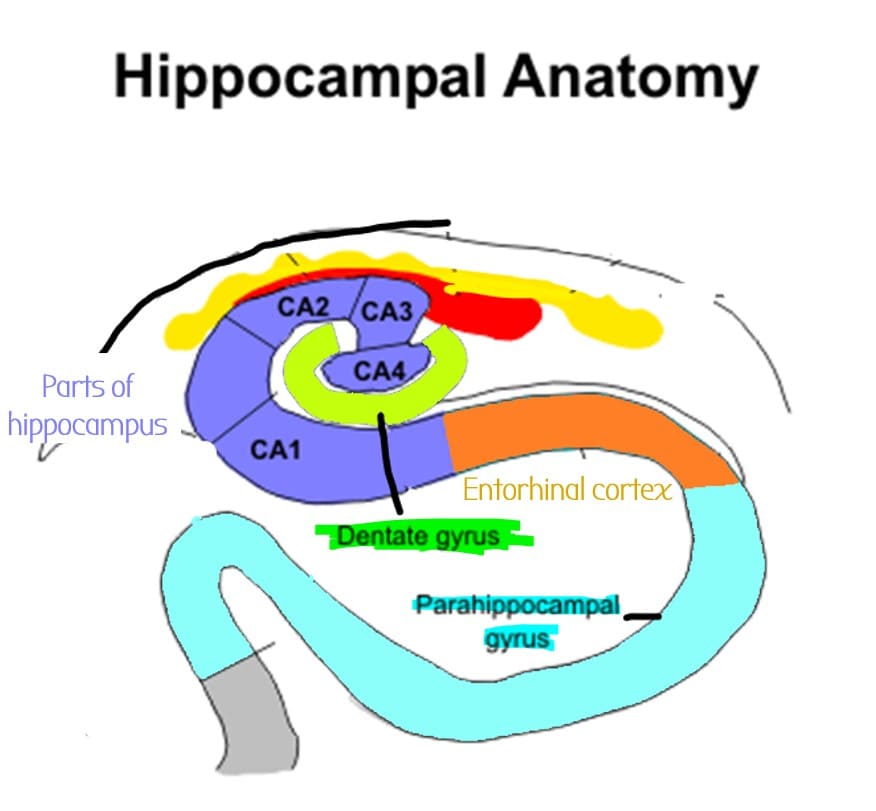
⚠️ If Hippocampus is involved in focal seizures, you get Deja-vu
Fornix
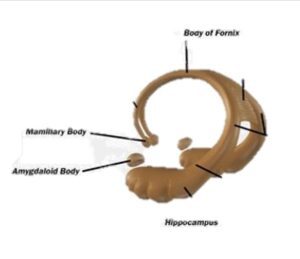
Tract of white matter that carries info into and out of hippocampus 🦛
It ends in two bulbs - the mamillary bodies which are part of the hypothalamus.
Fornix carries info out of hippocampus into the mamillary bodies
& Out of the septal nuclei in the mamillary bodies into the hippocampus.
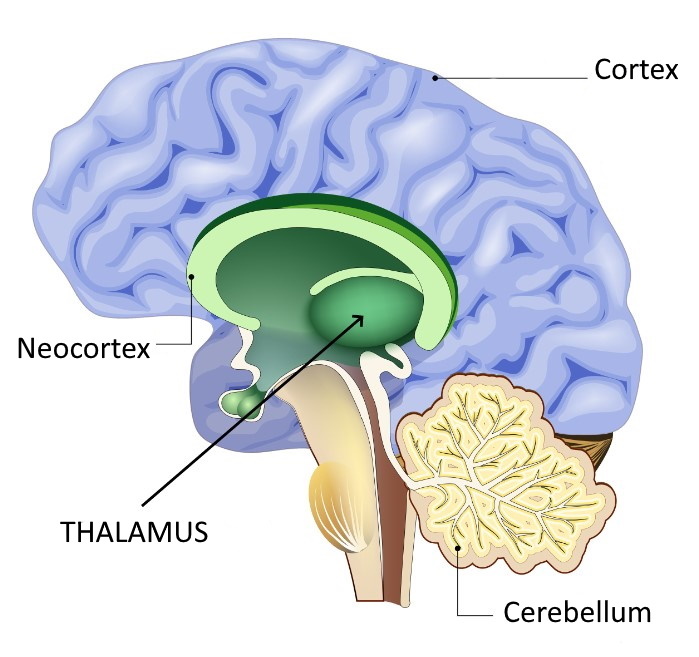
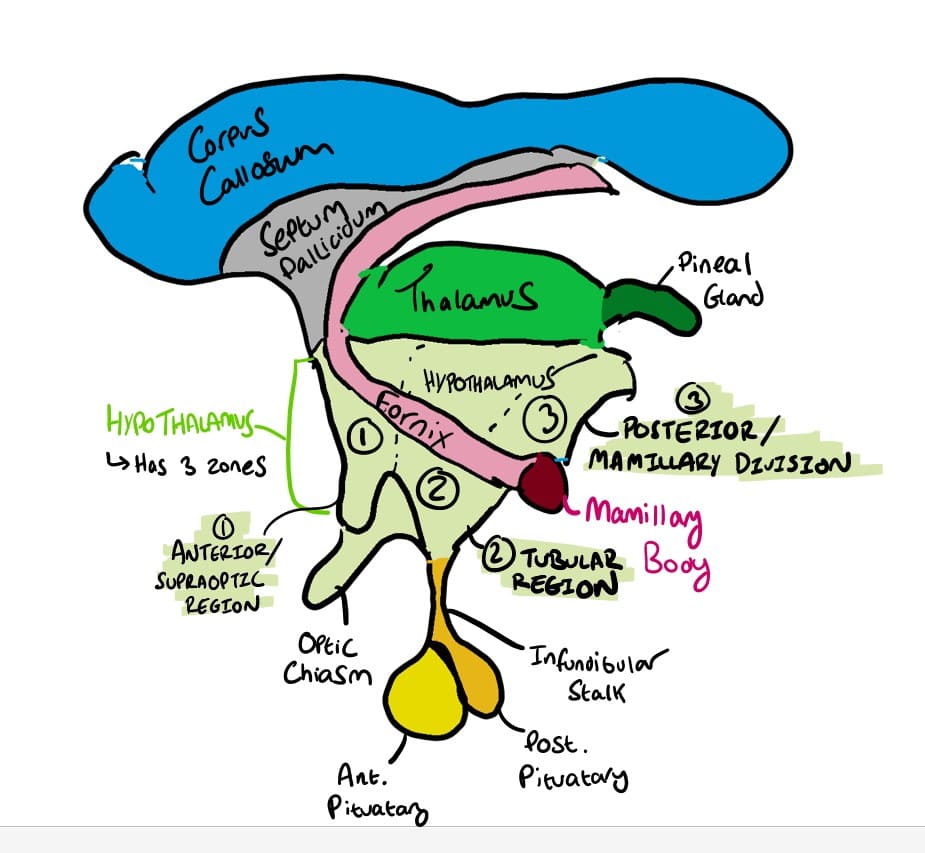
Hypothalamus
- Sits underneath thalamus
- Important for homeostasis
- Has three regions:
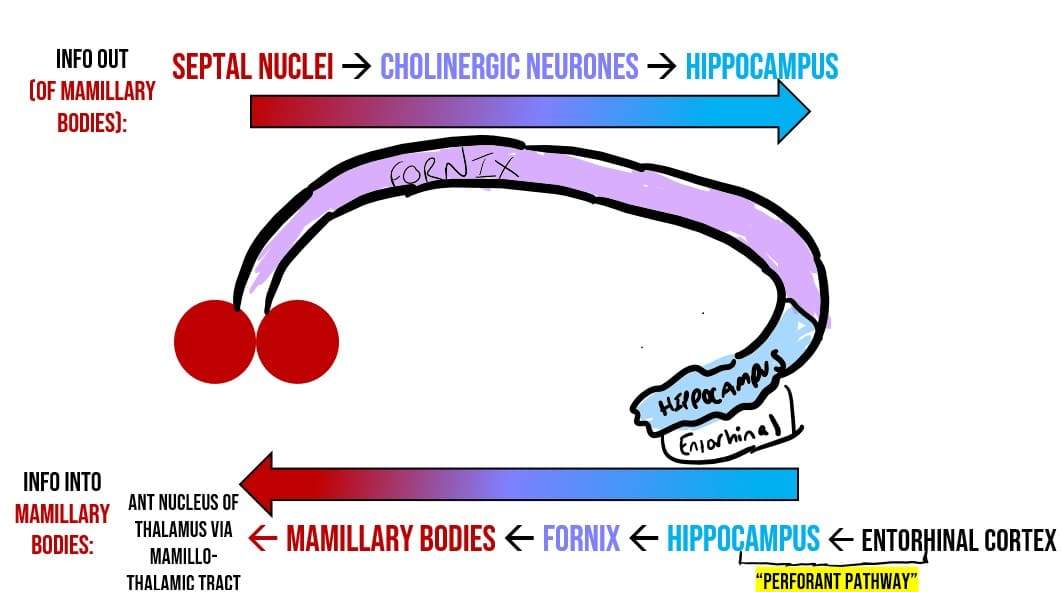
Info can enter hippocampus through:
- Perforant pathway
- Septohippocampal cholinergic neurones
Info out of hippocampus leaves via the fornix, goes to the mamillary bodies –> anterior nucleus of thalamus
Alzheimer’s disease: misfolded evil Tau proteins can spread from entorhinal cortex, through the hippocampus, then through the temporal lobe and then the neocortex
⚠️ If Hippocampus is involved in focal seizures, you get Deja-vu
HUNGRY/SLEEPY CONTROL ZONE
ARCUATE NUCLEUS:
- Controls Appetite by having leptin receptors (adipocytes release leptin to make you feel full/satiated)
- Fibres cross at midline here
- Also produces dopamine which acts to inhibit the release of prolactin (lactating hormone ) AKA DOMINANT NEGATIVE CONTROL
- ie Prolactin is basically always switched off (by dopamine) unless you are pregnant
- Therefore anti-psychotics that block D2 dopamine receptors (e.g. Risperidone, apomorphine) also stop arcuate nucleus from producing dopamine = lead to the side effect of high prolactin
- =hyperprolactinaemia! (can cause unwanted lactation)
TUBULAR MAMMILARY NUCLEUS:
- Tubular mamillary nucleus controls wakefullness.
- The only histamine nucleus in CNS.
- Therefore antihistamines can make you sleepy
- Area damaged in ENCEPHALITIS LETHARGICA – sleeping for upto 20hrs a day!
- The interlaminar nuclei of the thalamus also control sleepiness
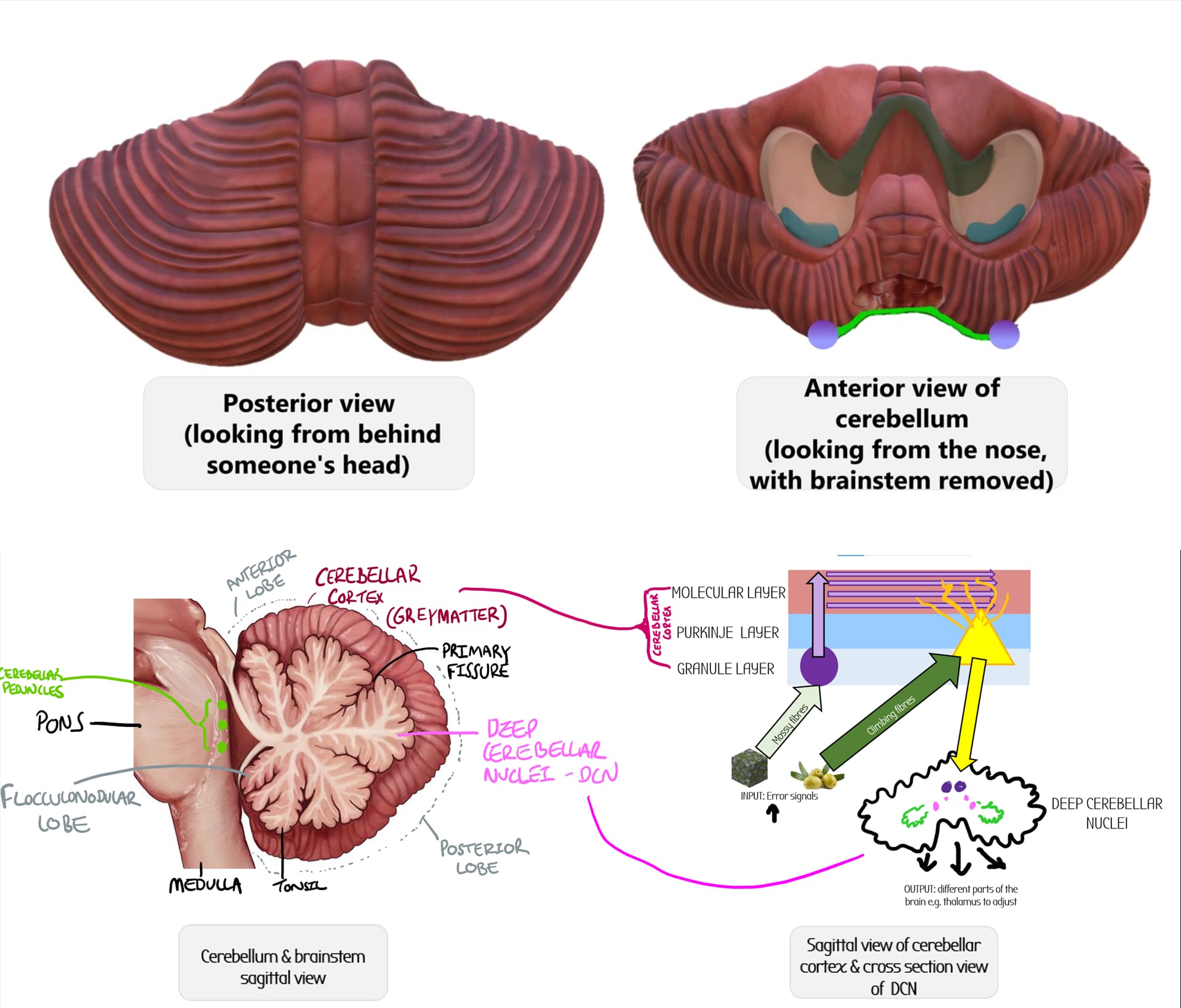
Vermis
Long worm thing that runs along the middle of the cerebellum, and separates the left and right hemispheres
Primary Fissure
Separates the anterior and the posterior lobes of the cerebellum
Anterior Lobe
-Consists of parts I-V (1-5) of the cerebellum
-Lesions in the anterior lobe lead to GAIT ATAXIA .
- The anterior lobe of the cerebellum can be damaged in alcoholics (in Korsakoff's syndrome)
- Alcohol = malabsoprtion of Vit B1 = brain damage e.g. anterior lobe of cerebellum
Posterior Lobe
-Consists of parts VI-IX (6-9) of the cerebellum
Superior cerebellar peduncle
-connects to pons
Middle cerebellar peduncle
-Biggest peduncle
- connects to pons
Inferior cerebellar peduncle
- connects to pons/open medulla
- Dorsospinal cerebellar tract enters cerebellum from here (proprioceptive)
Spinocerebellum
Along the vermis & intermediate zones
Receives info about proprioception
Function:
- Receive a lot of information from spinocerebellar tracts (e.g. conscious proprioception, discriminative touch, temperature, pain etc)
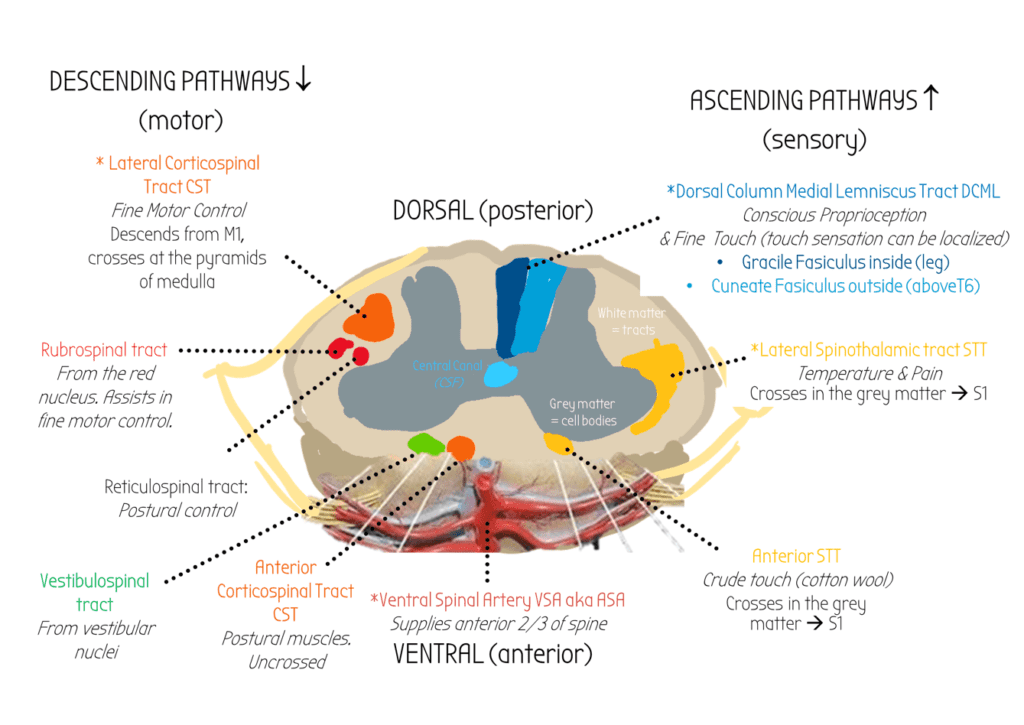
- Controls dorsolateral descending systems (rubrospinal and corticospinal)
- Adjust ongoing movement of whole body .
Anterior lobe vermis particularly sensitive to alcohol misuse. Lesions here can cause ataxia of gait
Lateral Lobes: pontocerebellum
Function:
Assist in fine movement control:
Influences motor (M1) and premotor (area 6) cortex via VENTROLATERAL NUCLES OF THALAMUS
SEND INFORMATION TO THE DENTATE NUCLEUS
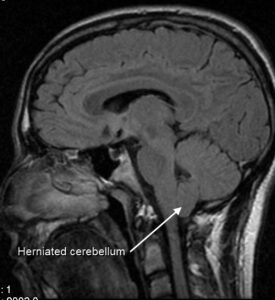
Cerebellar tonsil
Just above the floccular-nodular lobe there are two bumps at the lower surface of the cerebellm called the cerebellar tonsil.
These can herniate into the foramen magnum, and compress the medulla of the brainstem - breathing difficulties (chiari malformation).
Flocculus (part of the floccular-nodular lobe)
Anatomy:
-Part X (10) of the cerebellum
-At the very bottom of the cerebellum, visible from the inferior surface (you can barely see it from this view)
-The posterior lateral fissure divides the posterior lobes from the flocular-nodular lobes.
Function: Vestibulocerebellum
Controls balance & eye movement (eyes & ears!)
Damage = deficits in visual tracking , nystagmus (oscillation of eye movements), vestibulo-ocular reflex errors and balance problems
Cerebellar tonsil
Just above the floccular-nodular lobe there are two bumps at the lower surface of the cerebellm called the cerebellar tonsil.
These can herniate into the foramen magnum, and compress the medulla of the brainstem - breathing difficulties (chiari malformation).
Cerebelllar peduncles
Three masses of tissue that connect pons to the cerebellum.
Can be seen in cross section e.g. here:
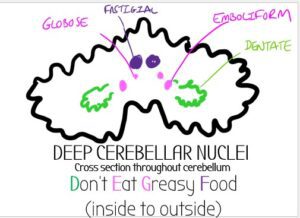
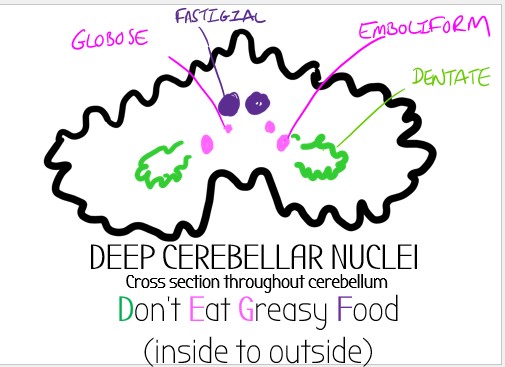
DCN
- 4 nuclei (dentate, emboliform & globose, fastigial)
- The cerebellar cortex projects to here via purkinje cells.
- These then go onto project to other parts of the brain
Climbing Fibres
- Carry Error Signals to the cerebellum e.g. retinal slip

- SOURCES:
- ALL ARISE FROM THE INFERIOR OLIVE

- Olive trees climb!
- ALL ARISE FROM THE INFERIOR OLIVE
- ROUTE:
- Fibres come from the inferior olivary nuclei in the olives in the medulla
- Cross the midline (CONTRALATERAL) and go to inferior cerebellar peduncle
- From here, they form climbing fibres
- These climb directly to the purkinje cell (without splitting into parallel fibres)
- PURKINJE CELL OUTPUT
- ONE CLIMBING FIBRE TO ONE PURKINJE CELL (1:1)
- Purkinje cell has one output fibre to the deep cerebellar nuclei to make adjustments
INPUT: Spinocerebellar tracts
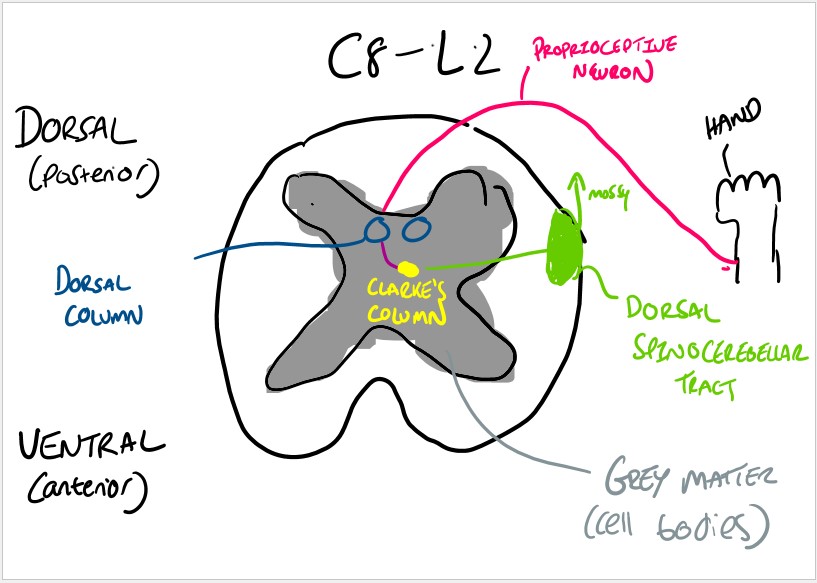
- These tracts contain proprioceptive info
- Info comes from proprioceptive neurones, which go to the dorsal column, synapse at Clarke’s column in the grey matter (Cell bodies)
- This neuron then goes to the white matter (tracts) and travels up the dorsal spinocerebellar tract
- The tract goes to the inferior cerebellar peduncle –> vermis
- Fibres becomes mossy fibres, then parallel fibres
- Project onto one purkinje cell –> Globose/Emboliform nuclei
OUTPUT:
- Controls dorsolateral descending systems (rubrospinal and corticospinal)
OUTPUT:
- Outputs information about planning movements to the Dentate Nucleus
- Dentate nucleus has efferent projections (outputs) which leave via the SUPERIOR CEREBELLAR PEDUNCLE
- These go to the ventrolateral nucleus of thalamus & crosses the midline
- The ventrolateral nucleus of the thalamus projects to the motor (M1) and premotor (area 6) cortex in the cerebrum
- The cerebrum sends these motor signals out via corticospinal tracts which cross at the pyramids
- Because there is double crossing, the cerebellum has ipsilateral motor control
From here, the error signals (mossy/climbing fibres) project onto Purkinje fibres which then output the error information to the FASTIGIAL NUCLEUS
floccular-nodular lobe
Project directly to
- vestibular nuclei in the dorsolateral medulla (supplied by PICA)
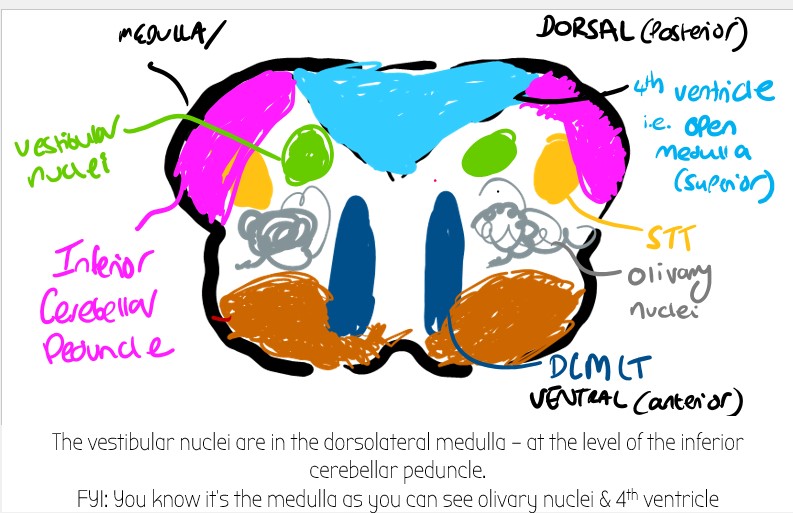
- Reticular formation
Input from ventral lateral/ventral anterior nucleus of thalamus
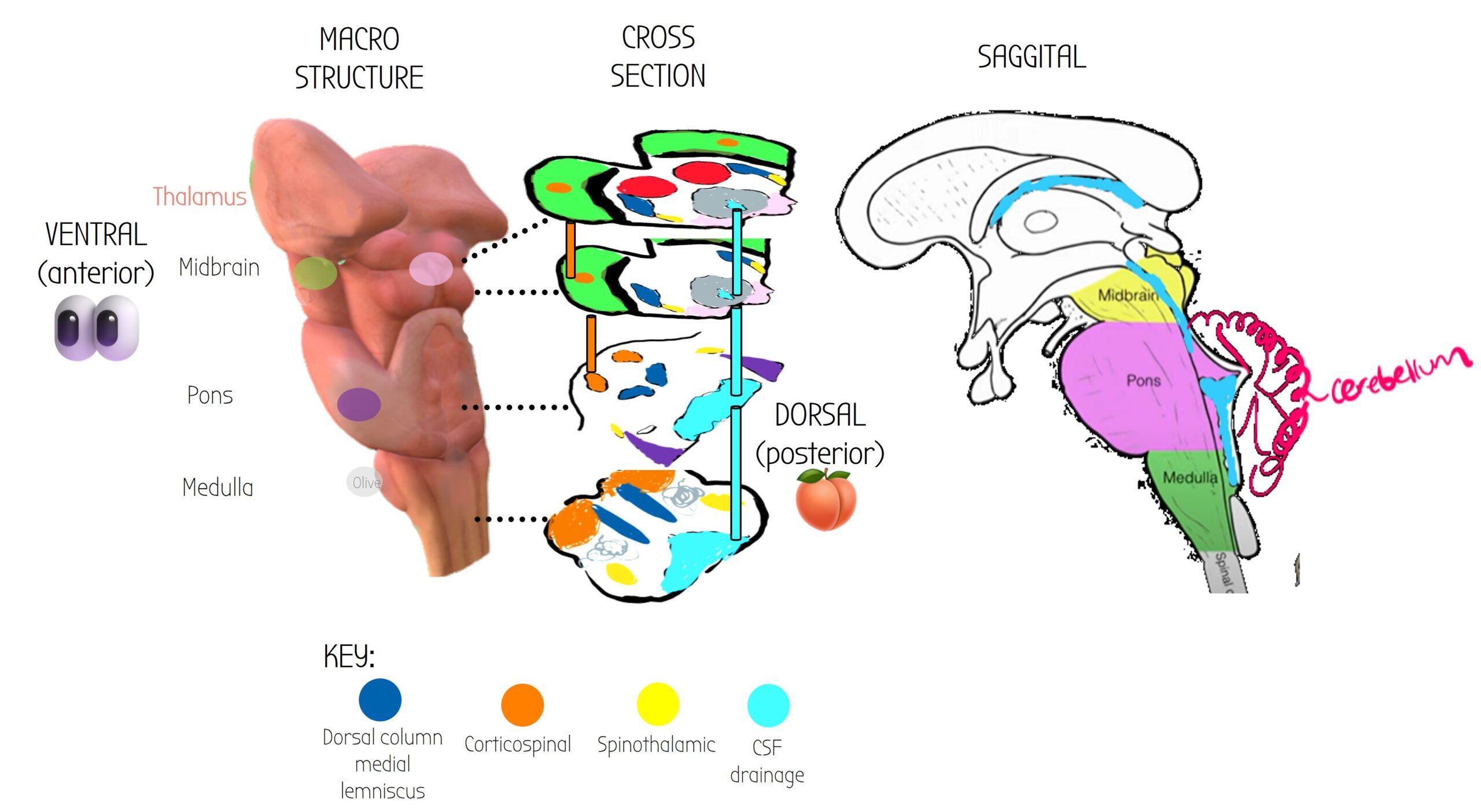
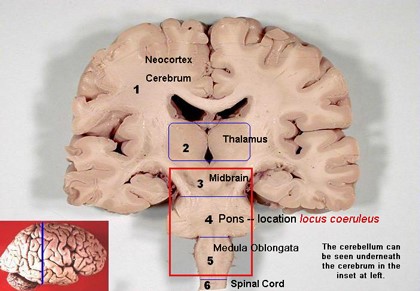
The brainstem is the bit of the brain that connects to the spinal cord – it is responsible for a lot of the non-conscious stuff that keeps us alive.
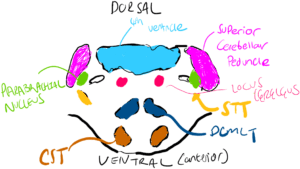
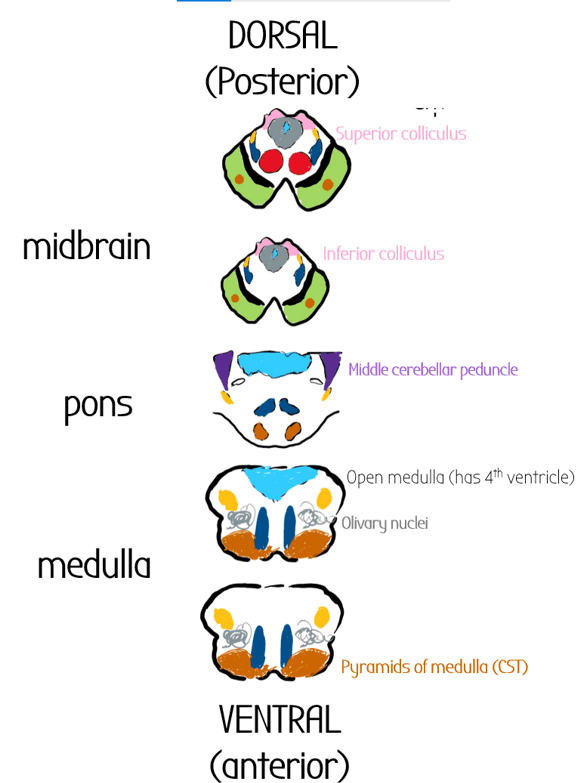
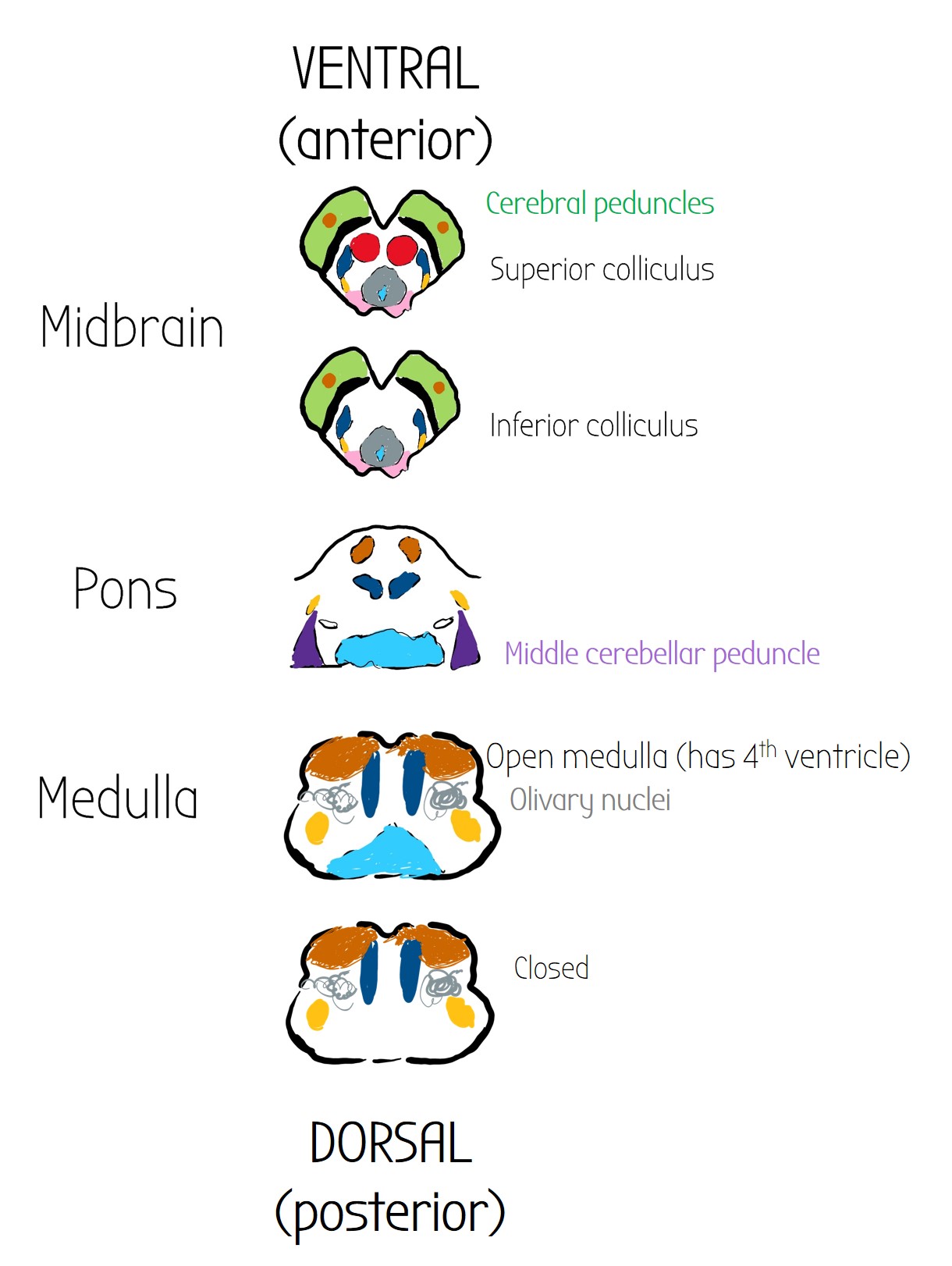
It is made of three sections:
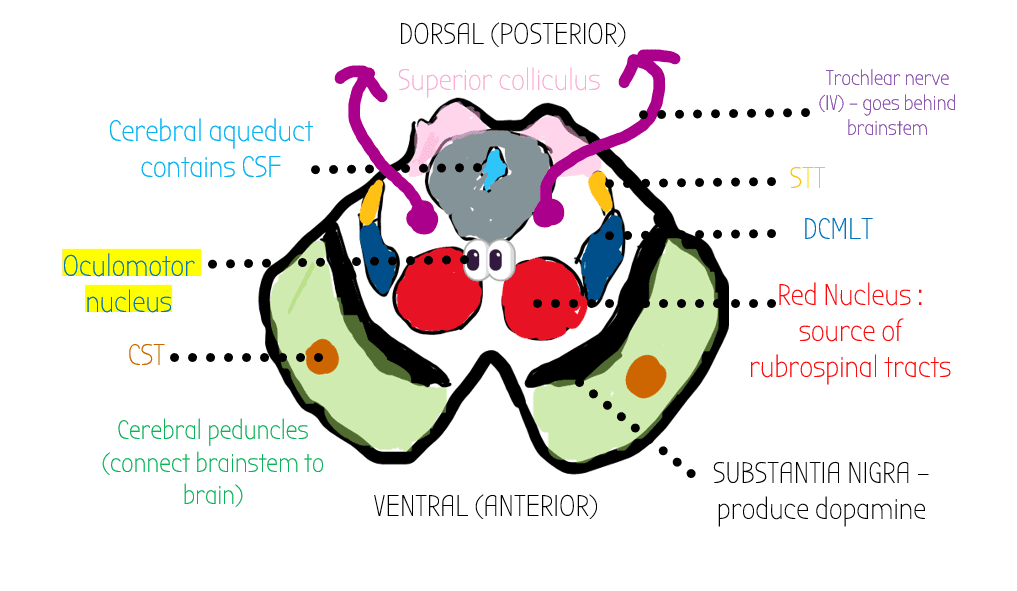
- Midbrain (aka mesencephalon): cerebral peduncles containing CST (shown in green), substantia nigra, red nucleus, DCMLT, STT, midbrain reticular formation, periaqueductal grey, superior/inferior colliculi
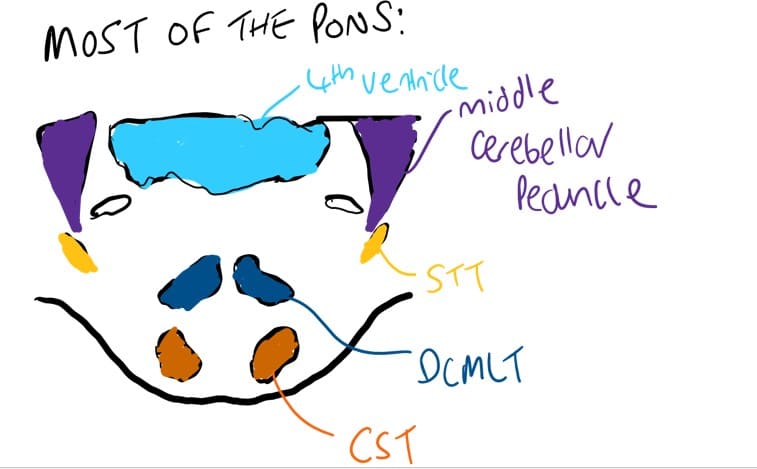
- Pons can be divided into layers based on the connections to the cerebellum (mini motor brain) called the cerebellar peduncles
- Superior cerebellar peduncles
- Middle cerebellar peduncles (these are the biggest)
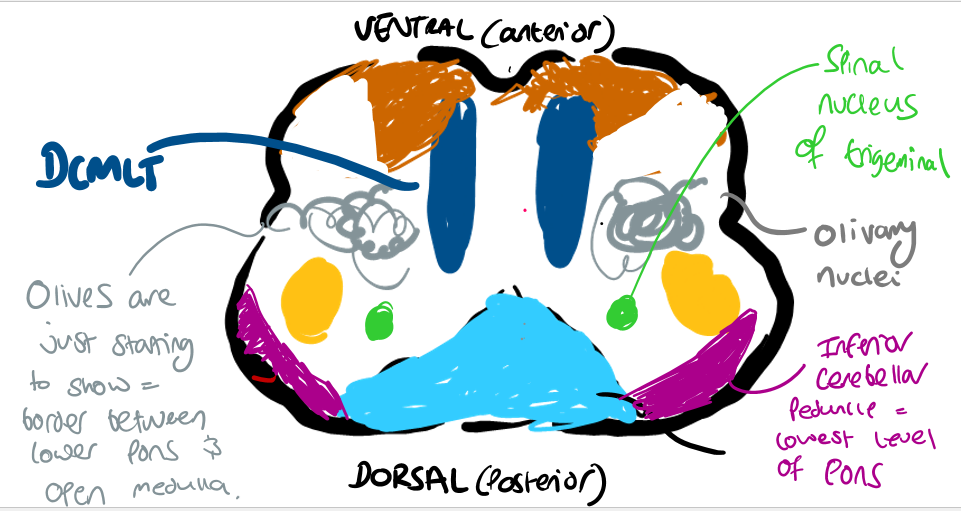
- Inferior cerebellar peduncles – most inferior bit of the pons
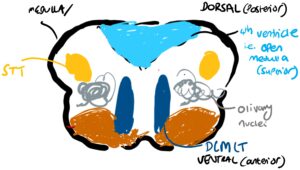
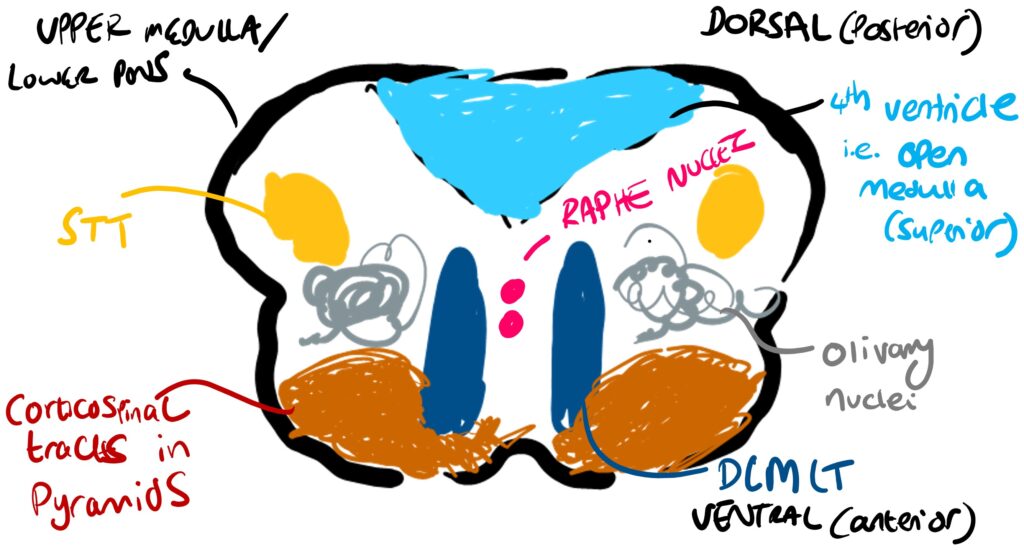
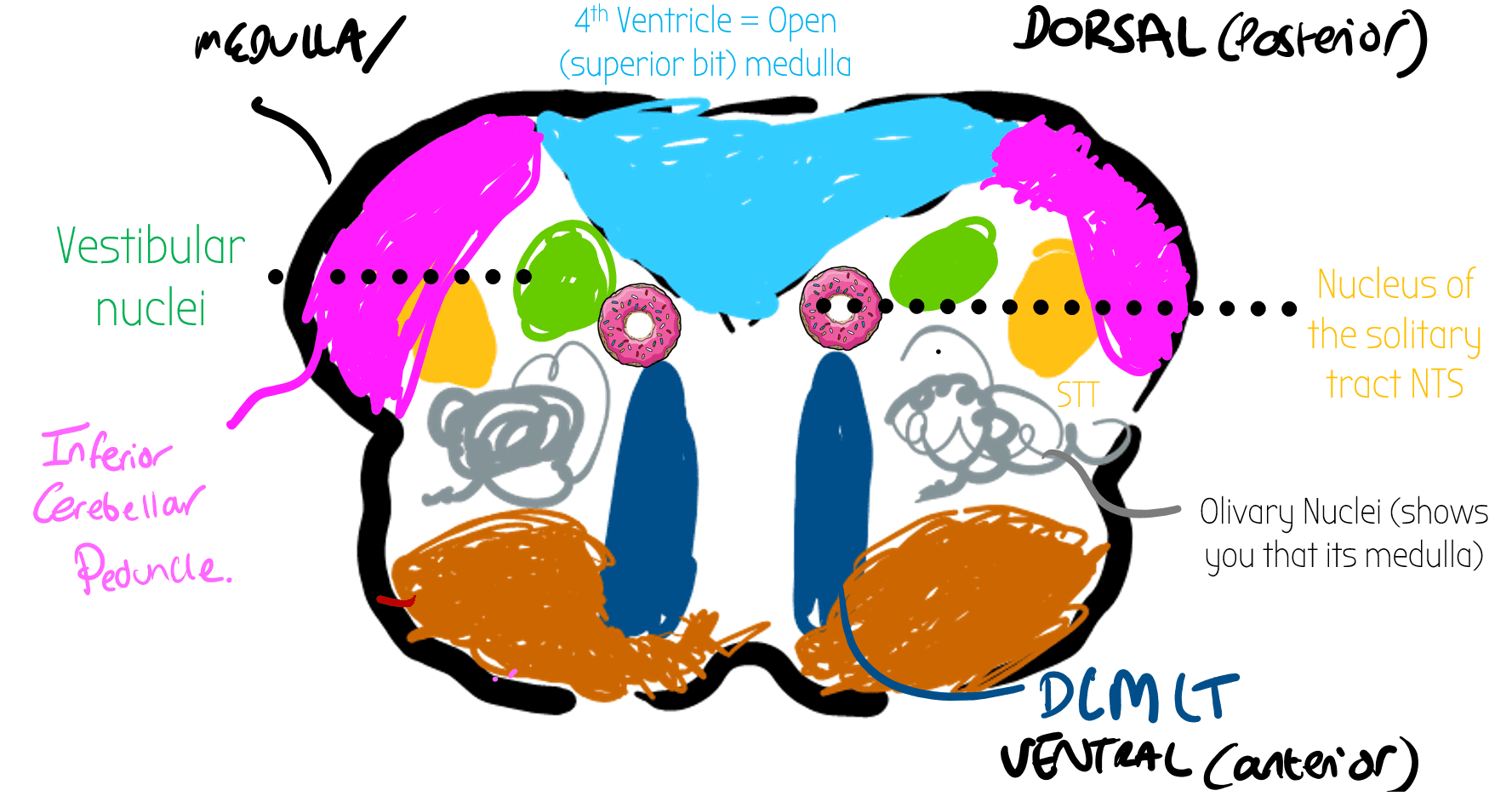
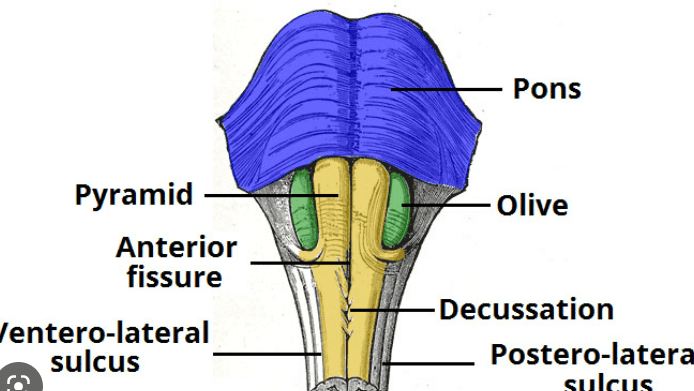
- Medulla the most inferior (caudal – closer to the spinal caud!) bit of the brainstem. Has distinct curly bits which are the olivary nuclei
- SUPERIOR: OPEN MEDULLA
 The upper bit of the medulla has the 4th ventricle (last collection of CSF in the brain) and is called the open medulla.
The upper bit of the medulla has the 4th ventricle (last collection of CSF in the brain) and is called the open medulla. - INFERIOR: CLOSED MEDULLA
 The 4th ventricle narrows in the lower bit of the medulla to become the central canal of the spinal cord. Therefore there is no more 4th ventricle/fluid stuff in the inferior bit of the medulla
The 4th ventricle narrows in the lower bit of the medulla to become the central canal of the spinal cord. Therefore there is no more 4th ventricle/fluid stuff in the inferior bit of the medulla
- SUPERIOR: OPEN MEDULLA
After the medulla is the spinal cord
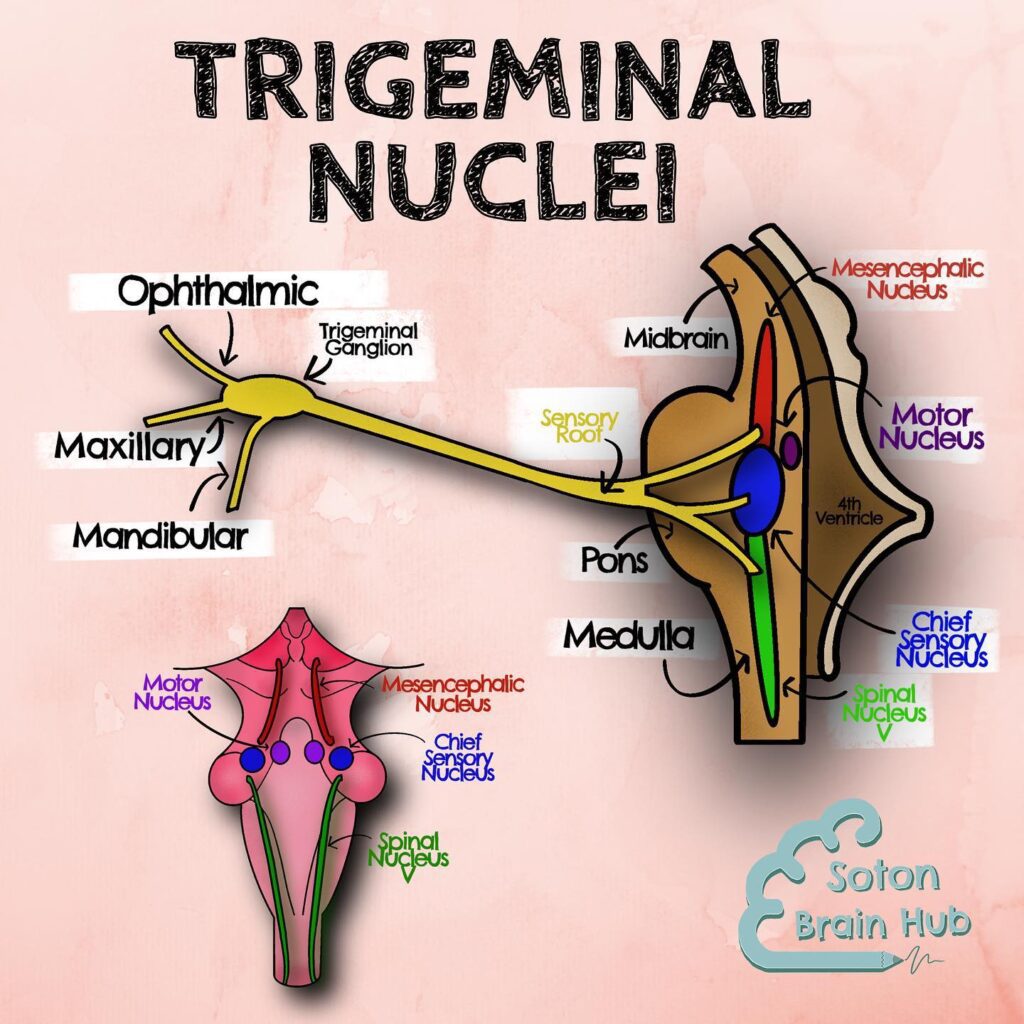
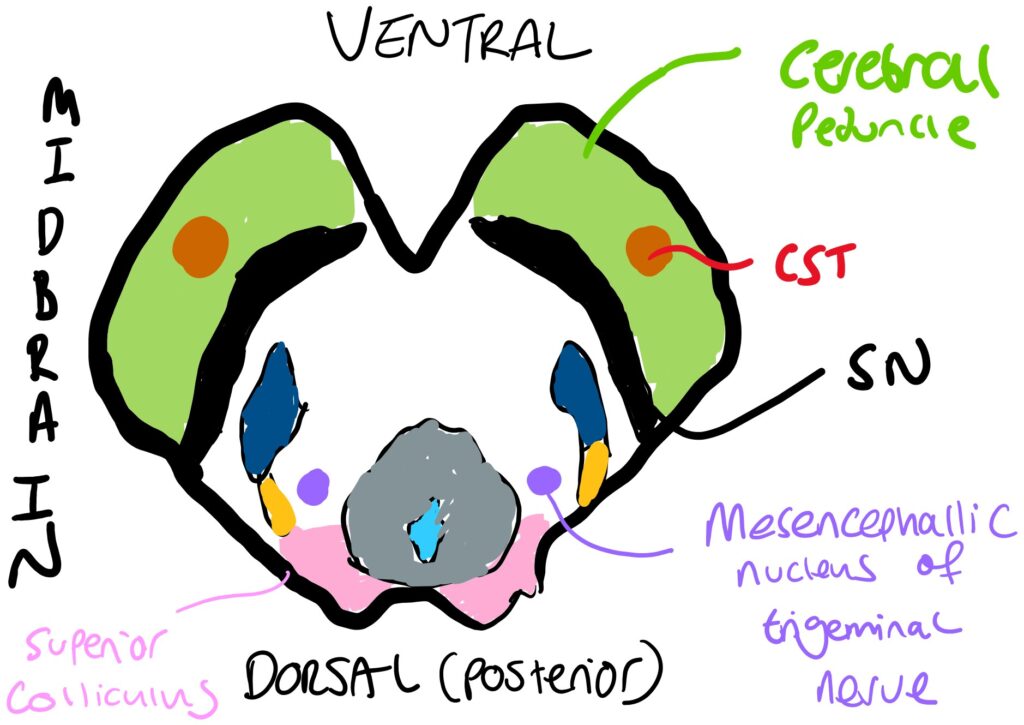
Spinal nucleus controls nociceptive (pain sensing) bits of trigeminal nerve via C fibres
 Anterior 2/3 of tongue supplies somatosensory information via lingual nerve (mandibular branch) to spinal nucleus
Anterior 2/3 of tongue supplies somatosensory information via lingual nerve (mandibular branch) to spinal nucleus
Found throughout brainstem.
Open medulla:
At the level of the open medulla, it contains internal arcuate fibres.
These fibres go to ventral posterior nucleus of thalamus (which is quite close to the brainstem). From here info gets relayed to somatosensory areas of cerebral cortex (e.g. post-central sulcus) via RECICIPIRICAL CONNECTIONS
The post central sulcus in the cerebrum helps work out what objects are via discriminative touch : STEROGNOSIS
Climbing Fibres
- Carry Error Signals to the cerebellum e.g. retinal slip
- SOURCES:
- ALL ARISE FROM THE INFERIOR OLIVE
- Olive trees climb!
- ALL ARISE FROM THE INFERIOR OLIVE
- ROUTE:
- Fibres come from the inferior olivary nuclei in the olives in the medulla
- Cross the midline (CONTRALATERAL) and go to inferior cerebellar peduncle
- From here, they form climbing fibres
- These climb directly to the purkinje cell (without splitting into parallel fibres)
- PURKINJE CELL OUTPUT
- ONE CLIMBING FIBRE TO ONE PURKINJE CELL (1:1)
- Purkinje cell has one output fibre to the deep cerebellar nuclei to make adjustments
Optic Chiasm Damage
Often due to pituitary adenoma (tumour of pituatary gland) - HIGH YIELD - ESR LINK!
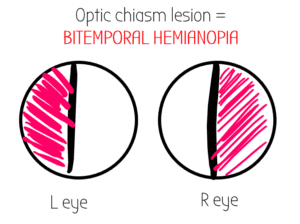
The outer visual fields (temporal fields) cross at the optic chiasm - so damage here causes loss of the lateral/outer/temporal fields
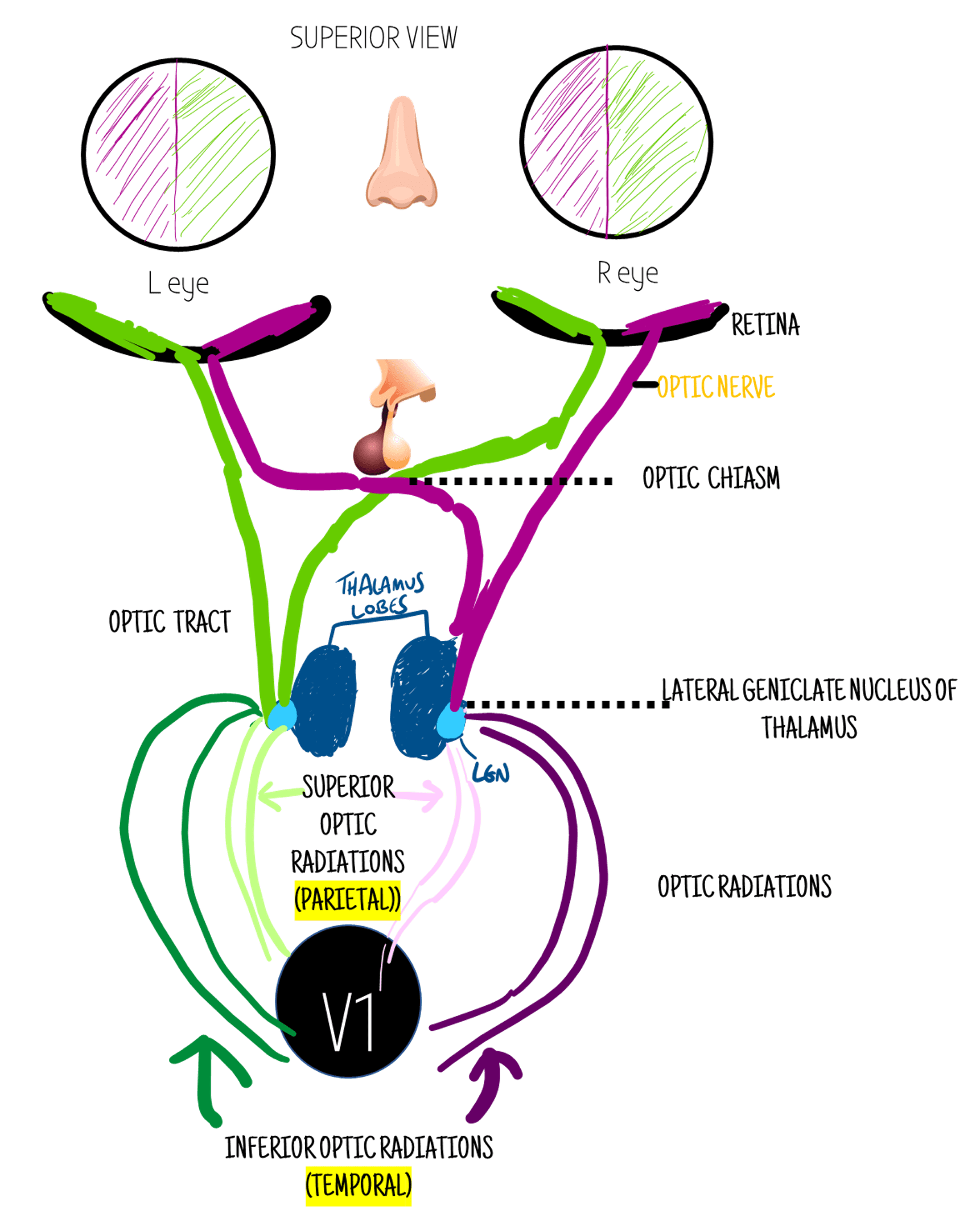
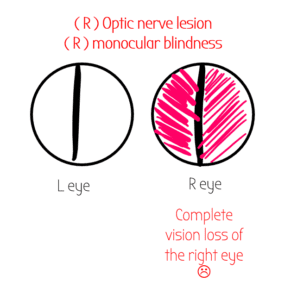
Optic Nerve
Info leaves the retina from both visual fields through a bundle of fibres called the optic nerve. The optic nerve then travels into the brain.
Each eye has its own optic nerve - CNII
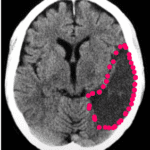
Occipital lobe/ V1 Lesion
Supplied by PCA
-PCA Stroke
This CT scan shows a stroke on the patient's LEFT side.
PCA stroke may also affect CNIII (oculomotor) - Weber's Syndrome
Optic Tract
The optic nerve turns into the optic tract after the optic chiasm.
The optic tract contains the visual info from the contralateral visual field - ie the left optic tract contains the info for the right visual field (green) - because of the crossing at the retina.
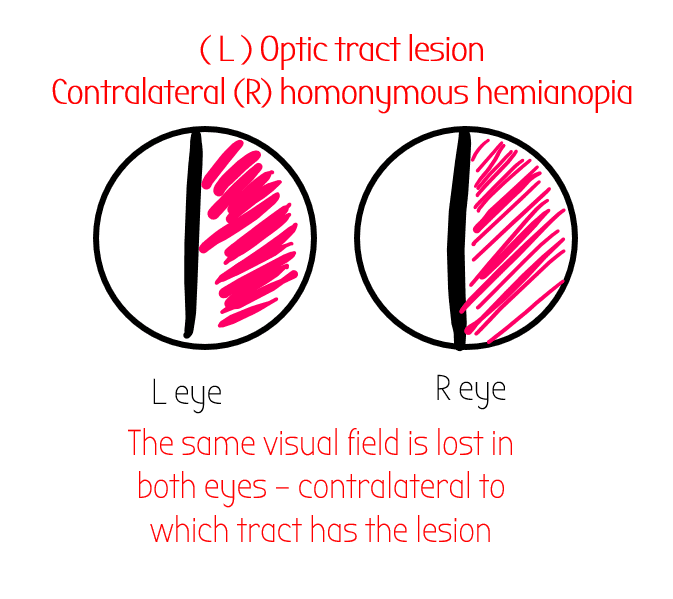
🩸 Optic tract lesions often occur in MCA strokes
Often occurs with Relative Afferent Pupillary
Defect
---> Test for by swinging the shining light. The patient should not normally have RAPD - it’s a bad thing!
Optic Radiations
After the optic tracts have gone to the thalamus, they split into 4 optic radiations - 2 superior/& 2 inferior branches.
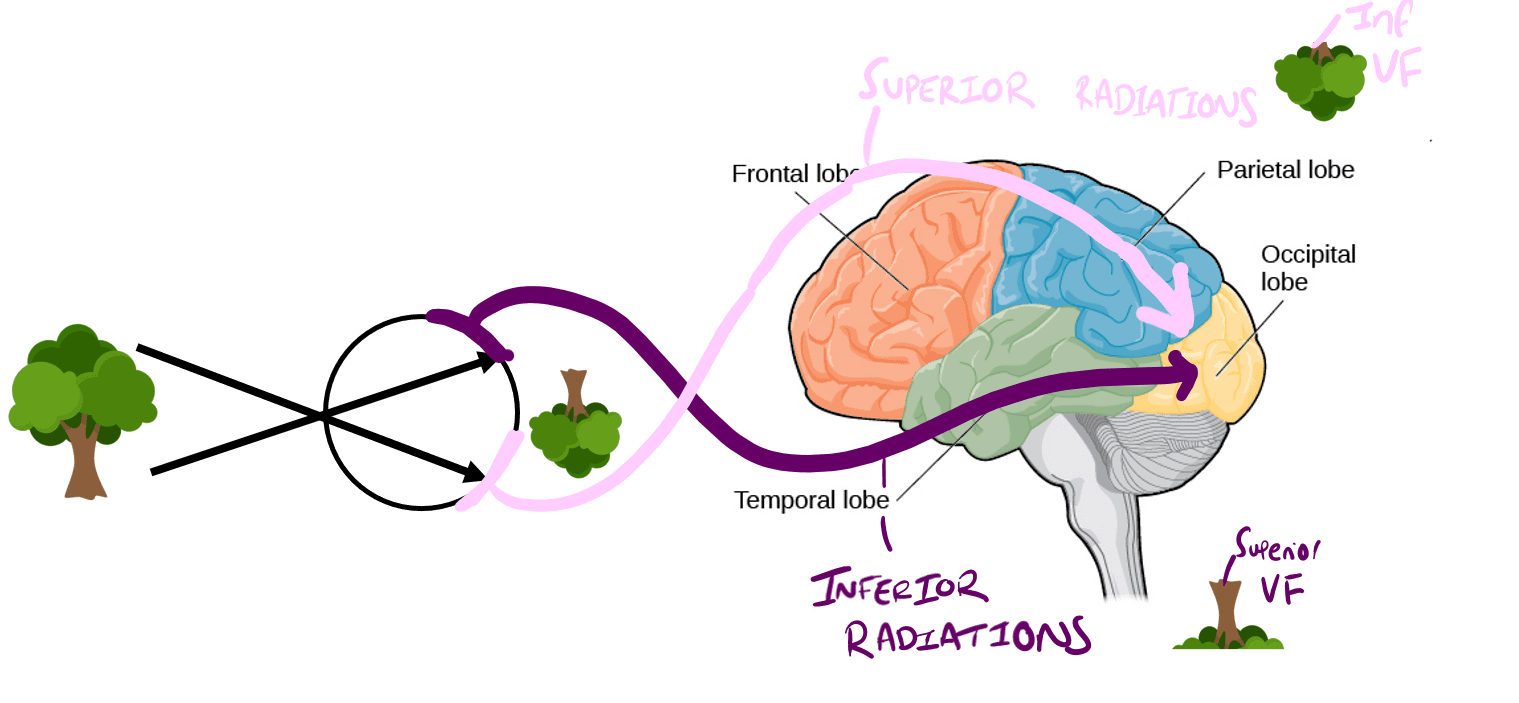
- Superior optic fibres pass over the parietal lobe - carry info about INFERIOR VF
- Inferior optic radiations - pass through temporal lobe - carry info about SUPERIOR VF
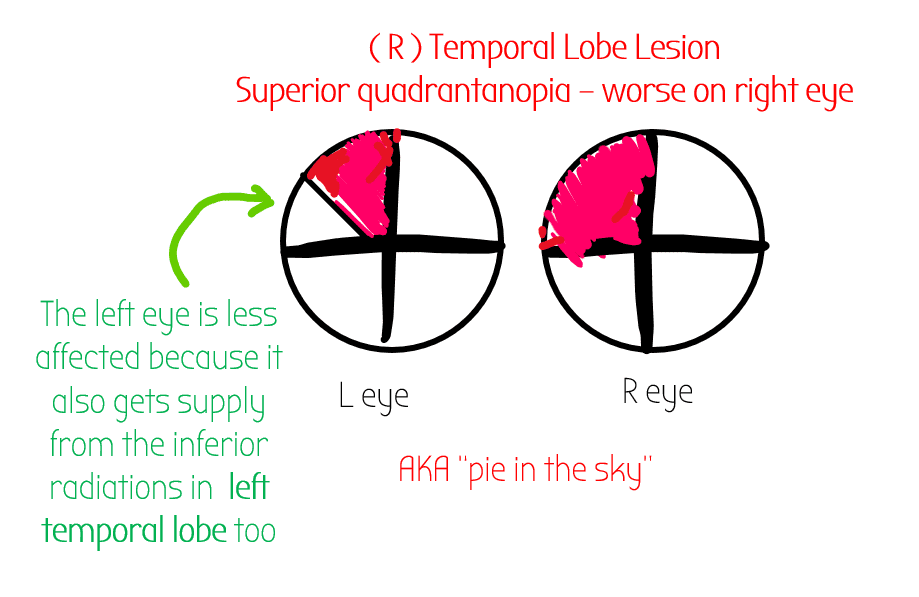
Inferior Optic Radiation
Come from LGN, go through the temporal lobe.
Contain info about the superior visual fields.
When the temporal lobe is damaged, you will get loss of the contralateral visual field BUT it will only be in the superior quadrant
Lesion in both superior and inferior optic radiations:
High yield tracts have a *
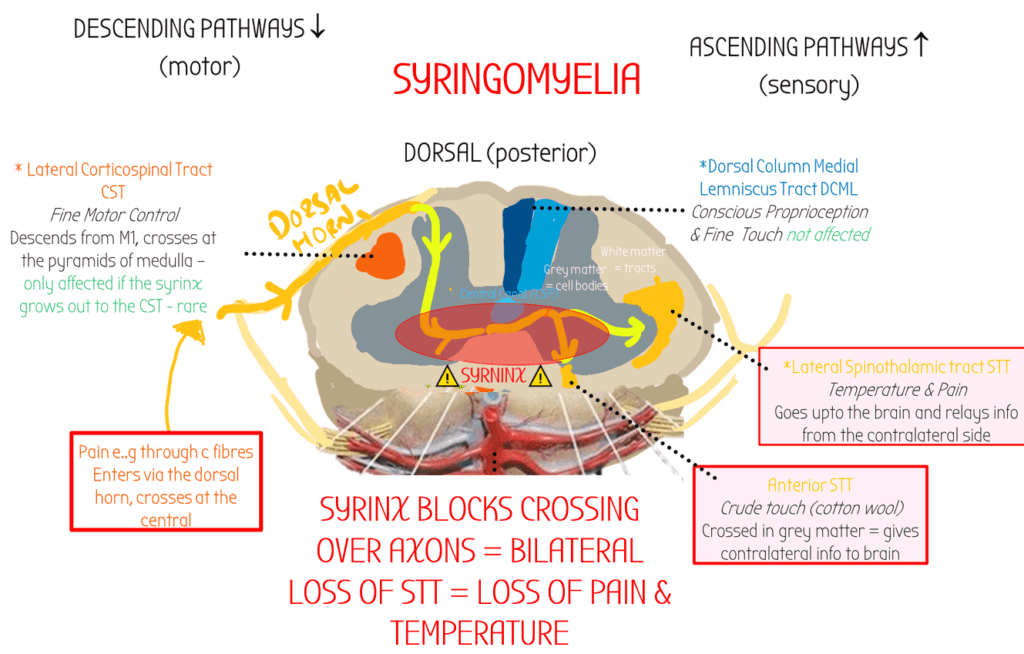
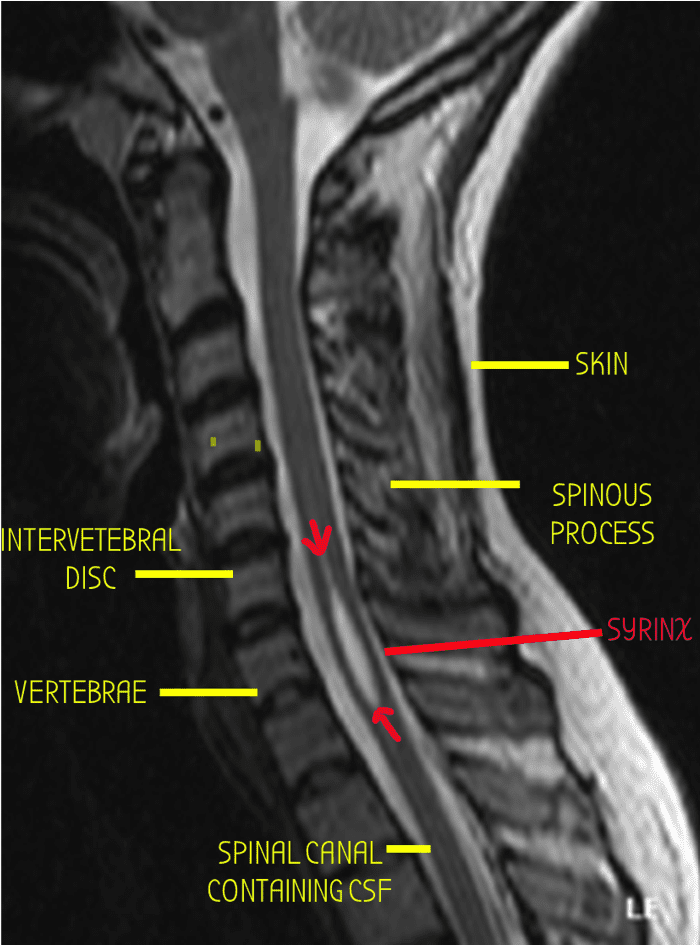
Syringomyelia occurs when a fluid filled cyst goes in the spinal central canal & blocks crossing over axons.
Complete loss of both nociceptive (spinothalamic) & proprioceptive (DCML) sensation at the level of the injury
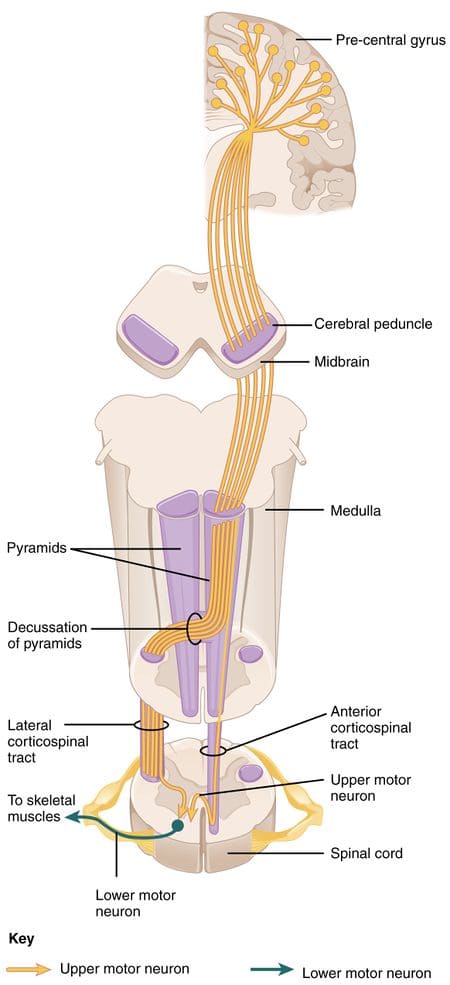
If (lateral) corticospinal tracts are damaged after they have crossed at the pyramids of the medulla, then symptoms will be IPSILATERAL (i.e. if damaged in the spine) . If damaged before they cross (in the brain/UMN), symptoms are contralateral
Strokes:
-PCA (contralateral hemiplegia – mostly in face)
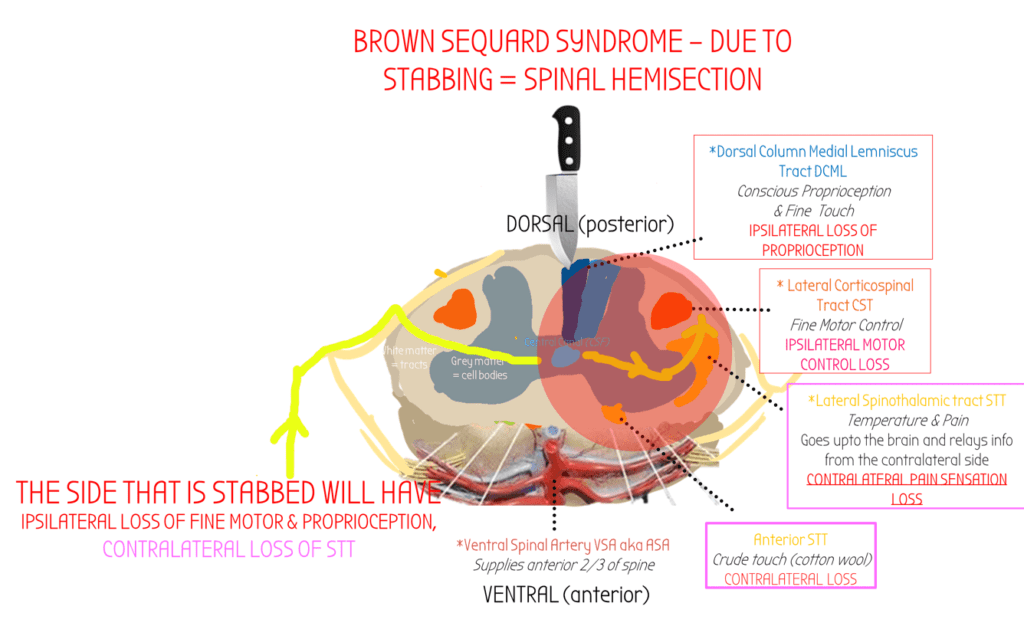
–Brown-Sequard Syndrome
Hemisection of spinal cord often due to stabbing
at the level of & below the lesion: IPSILATERAL fine motor los
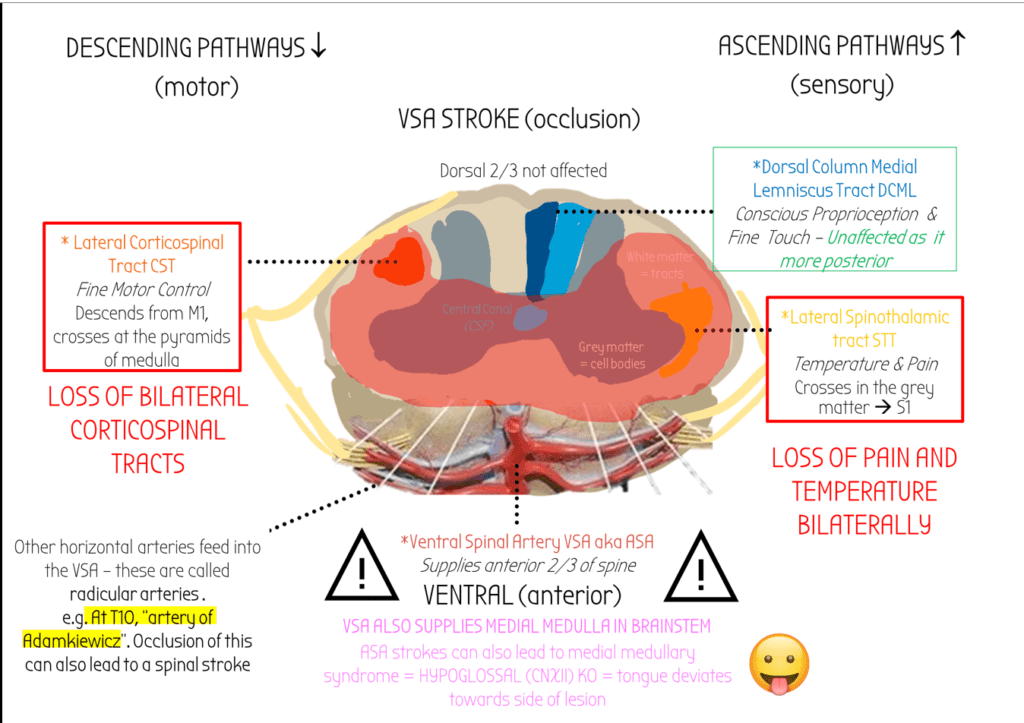
Ventral (anterior) Spinal Artery Stroke
–Syringomyelia rarely affects the CST – if the syrinx grows outwards to the lateral CST.
UMN ALWAYS INVOLVE CORTICOSPINAL TRACTS. LOSS OF CST IN UMN LESIONS CAUSES HYPERREFLEXIA
Pathway
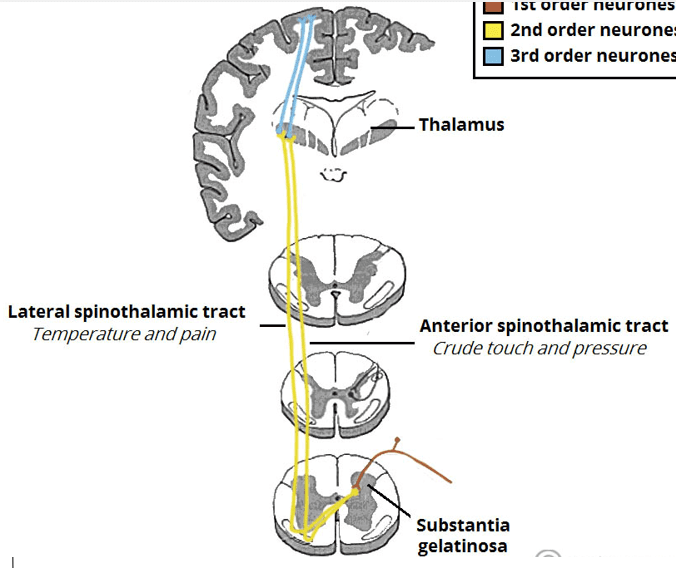
Pain/temperature info enters via the dorsal column, goes through the grey matter and crosses-over near the spinal canal, and then goes upto S1.
Therefore carries contralateral pain/nociception/temperature info
Pathway
Fibres go to the VP nucleus of the thalamus –> S1 somatosensory areas via reciprocal connections.